Pediatric Hip Stability Assessment



Pediatric Hip Stability Assessment
Congenital hip dislocation (CHD) is a condition that can occur in utero. Another name for this condition is “developmental dysplasia of the hip.” Hip instability is one of the most common abnormality in newborns. Approximately 1 in 10 have hip instability. The pathogenesis has been identified to be caused by abnormal formation of the hip joint during their early stages of fetal development. Flattened posteromedial femoral head, anteversion, and a shallow acetabulum can result in subluxation of the hip. Clinical presentation can include:
- Asymmetry of the thighs or gluteal folds
- Limitation of hip abduction
- Unequal femoral length (uneven knees = Galeazzi’s sign)
- Delayed motor development
This instability tends to worsen as a child grows. Approximately 20 – 30% are identified after 3 months of age. Prolonged and repeated dislocation can lead to greater incidence of hip osteoarthritis. This is why early diagnosis is critical.
The focus of this blog is on the clinical techniques used to identify this condition. These tests has been reported to be best performed in the first 3 months of life.
Telescoping (Piston) Sign 
This technique begins with the child supine with hip and knee flexed to 90°. A compression force is applied through the long axis of the femur followed by a distraction force (telescoping). A positive test is considered to be excessive movement relative to uninvolved hip. This is a subjective assessment and there is no data on the test sensitivity or specificity
 Ortolani Test
Ortolani Test
This technique is used to assess the ability to relocate the hip via a traction force with abduction. Thus, the child is in supine with the hips and knees at 90° of flexion. The clinician places his/her thumbs on the infant’s medial thigh and fingers on lateral thigh (fingertips on greater trochanter if hands are large enough). A firm traction force is applied to the thigh while gently abducting the leg. The goal is to anteriorly translate the femoral head into acetabulum. Reduction of hip may result in an audible click. The leg may appear to shorten as the femoral head goes into the socket. This test has a sensitivity of 7% and a specificity of 100%.
Barlow Test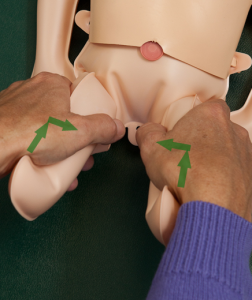
To the contrary, this technique is used to determine if the hip can be subluxed via compression with adduction. To identify this instability, place the child in supine with the hips and knees flexed at 90°. Like the Ortolani test, the clinician’s thumbs are on the infant’s medial thigh and fingers on the lateral thigh (fingertips on greater trochanter if hands are large enough). A posterior force is applied through the femur as the thigh is gently adducted 10-15 degrees. The clinician’s fingers on the greater trochanter will detect a palpable subluxation. The hip may go back into the socket when pressure is removed. This test has a sensitivity of 7% and a specificity of 100%.
Intervention
Fortunately, there is an effective treatment method. The Pavlik Harness uses hip flexion and free abduction to provide effective reduction in 91.5% of cases. This harness presses the hip joints into the sockets by securing the legs in a froglike position. The harness requires 3-6 months of continuous wear.
In a study performed between 2012 and 2014, 153 children (≤ 6 months of age) with developmental dysplasia of the hip were treated using the Pavlik harness. The threshold age value related to an increased risk of failure was found to be greater than or equal to 4 months old.
Success of Pavlik Harness treatment method decreases in children over 4 months of age. So the take-home message is that early identification and treatment are parameter.
For more cutting-edge orthopedic information on iOrtho+ PREMIUM Mobile App, please visit the learning modules at https://iortho.xyz/
If you would like to learn more about the Mobil-Aider orthopedic measurement device to quantify joint mobility, please visit: https://mobil-aider.com/
- Baronciani D, Atti G, Andiloro F, Bartesaghi A, Gagliardi L, Passamonti C, Petrone M. Screening for Developmental Dysplasia of the Hip: From Theory to Practice. Pediatrics. 1997;99(2):e5
- Gulick DT. iOrtho+ Premium Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- LeVeau B: Hip. In Richardson JK, Iglarsh ZA: Clinical orthopedic physical therapy, Philadelphia, 1994, W.B. Saunders.
- Magee D. Orthopedic Physical Assessment. 5th ed. Philadelphia, PA: WB Saunders Company; 2008.
- Ömeroğlu K, Akceylan I. Success of Pavlik Harness treatment decreases in patients greater than 4 months. Clinical Orthopaedics & Related Research 2015 June 6
- Ortolani M. The classic: Congenital hip dysplasia in the light of early and very early diagnosis. Clinical Orthopaedics & Related Research. 1976;119(2)
- Tachdjian MO: Pediatric Orthopedics, Philadelphia, 1972, WB Saunders