Hip Labral Tests



Hip Labral Tests
As we learn more about the structure and function of the hip labrum, we can appreciate the mechanism of injury and the clinical tests to identify pathology.
The labrum is a band of tough cartilage and connective tissue that lines the acetabular rim to deepen the hip socket. It cushions the hip joint and prevents the femoral head from rubbing against the acetabulum. Shearing forces from twisting and pivoting can damage the labrum. Excessive forces on the hip joint and acetabular impingement can tear the labrum which can lead to articular damage and hip destabilization. In addition, childhood disorders such as Legg-Calve-Perthes, hip dysplagia, and slipped capital femoral epiphysis (SCFE) increase the risk of labral injuries.
Symptoms associated can include any of the following: stiffness, clicking, popping, catching, and giving way. Patient will labral injuries often report dull aching with running, walking, and twisting motions. To be more specific, motions such as flexion, adduction, and internal rotation (IR) produce pain with anterior/superior tears and hyperextension, abduction, and external rotation (ER) will be painful with posterior tears.
Thus, there are at least 4 tests which utilize these motions in the differential diagnosis of the labrum: Anterior and Posterior Labral Tests, the Log Roll, and the Scour.
The anterior and posterior labral tests are also known as the Fitzgerald Tests. They use passive diagonal motions coupled with compression to capture the labrum.
The anterior labral test involves movement through a diagonal pattern. It begins in hip flexion, abduction, and ER and moves passively into extension, adduction, and IR. If you remem ber your PNF diagonals, it is very similar to a D2 extension pattern with the
ber your PNF diagonals, it is very similar to a D2 extension pattern with the  opposite rotational components. While moving through this diagonal, a longitudinal compressive force is applied through the femur to load the hip joint. A positive test could be a reproduction of pain in the hip or a clicking sensation.
opposite rotational components. While moving through this diagonal, a longitudinal compressive force is applied through the femur to load the hip joint. A positive test could be a reproduction of pain in the hip or a clicking sensation.
Similarly, the posterior labral test begins in hip flexion, adduction, and  IR and is passively taken into hip extension, abduction, and ER. Again, this resembles the PNF D1 extension pattern w
IR and is passively taken into hip extension, abduction, and ER. Again, this resembles the PNF D1 extension pattern w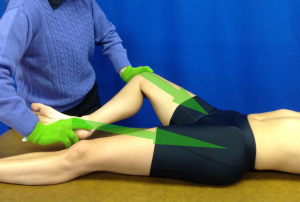 ith the rotational components switched. A positive test could be a reproduction of pain in the hip or a clicking sensation. The statistics for both these tests reveal they are good screening tools.
ith the rotational components switched. A positive test could be a reproduction of pain in the hip or a clicking sensation. The statistics for both these tests reveal they are good screening tools.
The metrics are as follows:
- Sensitivity = 75-100%
- Specificity = 43%
- (+) Likelihood ratio = 1.32
- (-) Likelihood ratio = 0.58
- (+) Predictive value = 100%
- (-) Predictive value = 0%
 The Log Roll Test is a rather nonspecific hip test. In addition to assessing labral lesions, it has been reported to be used to assess iliofemoral ligament laxity and hip impingement. The log roll test has also been used for a pediatric disorder of unknown etiology called phantom hip disease (AKA transient & toxic hip synovitis). Some literature has associated phantom hip disease with a prodromal upper respiratory infection. It has been reported in pre-pubescent children: they wake up in the morning and don’t want to move or put weight on their leg. Radiographs may be taken to rule out a slipped capital epiphysis but will be unremarkable.
The Log Roll Test is a rather nonspecific hip test. In addition to assessing labral lesions, it has been reported to be used to assess iliofemoral ligament laxity and hip impingement. The log roll test has also been used for a pediatric disorder of unknown etiology called phantom hip disease (AKA transient & toxic hip synovitis). Some literature has associated phantom hip disease with a prodromal upper respiratory infection. It has been reported in pre-pubescent children: they wake up in the morning and don’t want to move or put weight on their leg. Radiographs may be taken to rule out a slipped capital epiphysis but will be unremarkable.
To perform the log roll test, the patient is in supine with the legs extended. The clinician simply applies a force from medial to lateral to roll the thigh into maximal ER. Excessive ER, as compared to the contralateral side, may indicate iliofemoral ligament laxity. Pain may indicate a labral tear, impingement, or phantom hip disease in a child. Sensitivity is 30% and specificity has not been reported. Thus, this test may have limited value for differential diagnosis.
 The scour test mimics the technique of scrubbing a soiled pan. The repetitive, slow-amplitude, circular motions, combined with an axial load through the femur, incriminates the acetabular labrum. This motion is done in 90 degrees of hip and knee flexion to “capture” the labrum. If the labrum is captured, the client may experience a click, a grinding sensation, or pain. A false positive may be obtained if a client has osteoarthritis.
The scour test mimics the technique of scrubbing a soiled pan. The repetitive, slow-amplitude, circular motions, combined with an axial load through the femur, incriminates the acetabular labrum. This motion is done in 90 degrees of hip and knee flexion to “capture” the labrum. If the labrum is captured, the client may experience a click, a grinding sensation, or pain. A false positive may be obtained if a client has osteoarthritis.
The statistical data for this test is:
- Sensitivity = 88-100%
- Specificity = 43%
- (+) Likelihood ratio = 1.54
- (-) Likelihood ratio = 0.28
- (+) Predictive value = 23-100%
- (-) Predictive value = 95%
In summary, the combination of mechanism of injury, clinical signs and symptoms, as well as a positive labral test will help identify a labral concern. More evidence-based information and videos of these tests can be found in iOrtho+ Premium Mobile App. Past blogs and learning modules can be accessed at https://iortho.xyz/
- Burgess RM, Rushton A, Wright C, Daborn C. The validity and accuracy of clinical diagnostic tests used to detect labral pathology of the hip: A systematic review. Manual Therapy 2011;16: 318-326.
- Byrd JWT, Jones KS. Traumatic rupture of the ligamentum teres as a source of hip pain. Arthroscopy: Journal of Arthroscopic & Related Surgery. 2004;20(4):385-391
- Clohisy JC, Knaus ER, Hunt DM, Lesher JM, Harris-Hayes M, Prather H. Clinical Presentation of Patients with Symptomatic Anterior Hip Impingement. Clinical Orthopaedics & Related Research. 2009;467(3):638-644
- Fitzgerald RH Jr. Acetabular labrum tears: diagnosis & treatment. Clinical Orthopedics. 1995;311:60-68
- Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskeletal Med. 2009; 2:105 – 117
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Leiboid M, Huijbregts P, Jensen R. Concurrent Criterion-Related Validity of Physical Examination Tests for Hip Labral Lesions: A Systematic Review. The Journal of Manual Manipulative Therapy. 2008;16(2):E24-41.
- Martin RL, Sekiya JK. The interrater reliability of 4 clinical tests used to assess individuals with musculoskeletal hip pain. Journal Orthopedics Sports Physical Therapy. 2008 Feb;38(2):71-77
- Narvani A, Tsirdis E, Kendall S, Chaudhuri R, Thomas P. A preliminary report on prevalence of acetabular labral tears in sports patients with groin pain. Knee Surgery Sports Traumatology Arthroscopy. 2003;11:403-408
- Spring BA, Gill NW, Freedman BA, Ross AE, Javernick MA, Murphy KP. Acetabular labral tears: Diagnostic accuracy of clinical examination by a physical therapist, orthopedic surgeon, & orthopedic residents. North American Journal of Sports Physical Therapy. 2009;4(1):38-45