Assessing Leg Length


Assessing Leg Length
Just because we CAN do something does not mean we SHOULD!
The assessment of a leg length discrepancy is somewhat controversial. Some see the value in the assessment while others see the margin of error in the measurement. There are at least 3 methods used to assess leg length:
- Galeazzi Test
- Weber-Barton Maneuver
- ASIS to malleolus

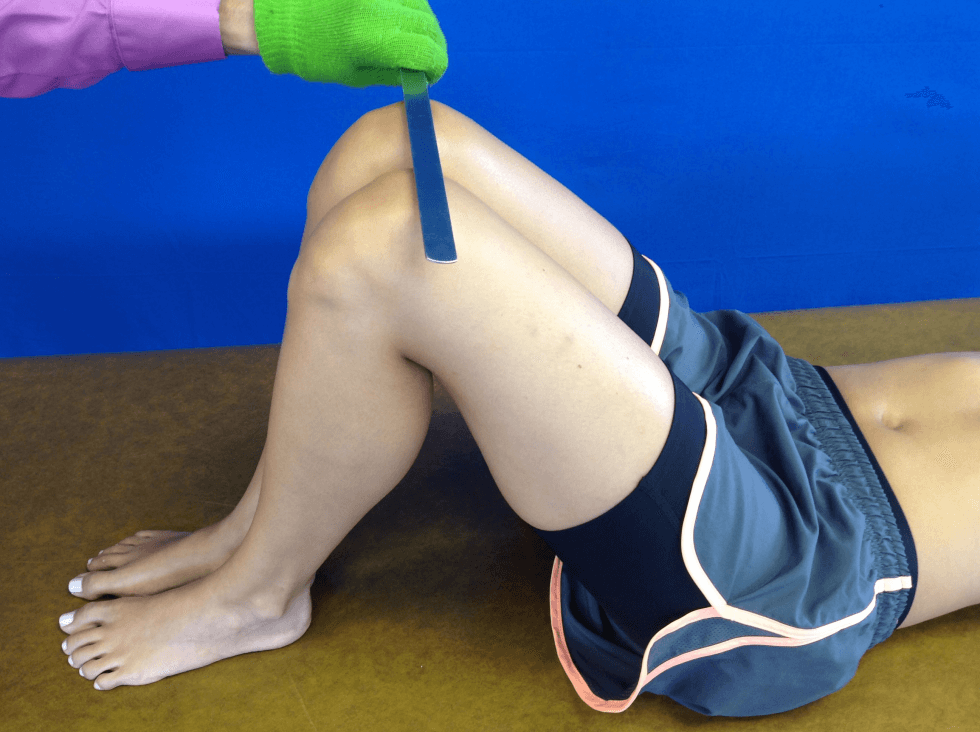
 The Galeazzi Test is also known as the Allis Sign and the Skyline Test. This test is performed in supine. The client’s hip and knee is passively flexed to approximately 45 and 90 degrees, respectfully. The medial malleoli are placed together. If the tibial tuberosities are not even, femur length may be asymmetrical (image left). Whereas, if anterior aspect of the distal knees are not level in height, tibial length may be asymmetrical (image right). This technique provides a general overview of where a leg length discrepancy may be attributed but it does not quantify it.
The Galeazzi Test is also known as the Allis Sign and the Skyline Test. This test is performed in supine. The client’s hip and knee is passively flexed to approximately 45 and 90 degrees, respectfully. The medial malleoli are placed together. If the tibial tuberosities are not even, femur length may be asymmetrical (image left). Whereas, if anterior aspect of the distal knees are not level in height, tibial length may be asymmetrical (image right). This technique provides a general overview of where a leg length discrepancy may be attributed but it does not quantify it.
 The
The  Weber-Barston Maneuver, also know as the Fitzgerald Test does permit quantification. The test is performed in supine. The client performs a bridging maneuver and then the clinician simultaneously, passively extends the client’s legs. The levels of the medial malleoli are compared. A test is considered positive if the leg length discrepancy is > 1.0 – 1.5 cm.
Weber-Barston Maneuver, also know as the Fitzgerald Test does permit quantification. The test is performed in supine. The client performs a bridging maneuver and then the clinician simultaneously, passively extends the client’s legs. The levels of the medial malleoli are compared. A test is considered positive if the leg length discrepancy is > 1.0 – 1.5 cm.

 Leg length discrepancy can also be assessed through the measurement of the distance from the ASIS to the malleolus. The client assumes a supine position and a bilateral traction force is applied to the lower extremities to equilibrate the pelvis. Option #1 is to measure from the prominence of the ASIS to the distal medial malleolus. While option #2 is to measure from the prominence of the ASIS to the distal lateral malleolus. A (+) test is > 1.0-1.5 cm difference between legs can be symptomatic. Leg length discrepancy may be due to a plethora of issues including but not limited to pelvic obliquity, coxa varus/valgus, and genu varus/valgus. One should also be aware of the errors that can occur in the assessment of leg length. For example, if the measurement is taking to the medial malleolus and there is a significant amount of unilateral lower extremity swelling or noteworthy quadriceps atrophy, the measure could be asymmetrical but have nothing to due with leg length. Accurate palpation of the anatomic structures and consist use of the same landmarks can also impact the precision of the leg length measurement.
Leg length discrepancy can also be assessed through the measurement of the distance from the ASIS to the malleolus. The client assumes a supine position and a bilateral traction force is applied to the lower extremities to equilibrate the pelvis. Option #1 is to measure from the prominence of the ASIS to the distal medial malleolus. While option #2 is to measure from the prominence of the ASIS to the distal lateral malleolus. A (+) test is > 1.0-1.5 cm difference between legs can be symptomatic. Leg length discrepancy may be due to a plethora of issues including but not limited to pelvic obliquity, coxa varus/valgus, and genu varus/valgus. One should also be aware of the errors that can occur in the assessment of leg length. For example, if the measurement is taking to the medial malleolus and there is a significant amount of unilateral lower extremity swelling or noteworthy quadriceps atrophy, the measure could be asymmetrical but have nothing to due with leg length. Accurate palpation of the anatomic structures and consist use of the same landmarks can also impact the precision of the leg length measurement.
Thus, if one desires to assess leg length, the technique selected may be significant, the presence of signs/symptoms, and the magnitude to which a correction should be considered. For more cutting edge orthopedic information via iOrtho+ Premium Mobile App, please visit https://iortho.xyz/
- Bolz S, Davies GJ: Leg length differences and correlation with total leg strength, J Orthop Sports Phys Ther 1984;6:123-129
- Clarke GR: Unequal leg length: An accurate method of detection and some clinical results, Rheumatol Phys Med. 1972; 11:385-390.
- Fisk JW, Balgent ML: Clinical and radiological assessment of leg length, N Z Med J. 1975; 81:477-480
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Magee D. Orthopedic Physical Assessment. 5th ed. Philadelphia, PA: WB Saunders Company; 2008.
- Reider B: The orthopedic physical examination, Philadelphia, 1999, W.B. Saunders.
- Sawyer JR, Kapoor M. The limping child: a systematic approach to diagnoses. American Family Physician. 2009;79(3):219
- Woerman AL, Binder-Macleod SA: Leg-length discrepancy assessment: Accuracy and precision in five clinical methods of evaluation, J Orthop Sports Phys Ther 1984;5:230-239
- Woerman AL: Evaluation and treatment of dysfunction in the lumbar-pelvic-hip complex. In Donatelli R, and Wooden MJ (eds): Orthopedic physical therapy, Edinburgh, 1989, Churchill Livingstone.