Elbow Joint Mobilizations
Elbow Joint Mobilizations


Elbow Injuries
When one thinks of elbow injuries, lateral epicondylitis, epicondylosis, and/or eipcondylalgia comes to mind. Perhaps you know this better as tennis elbow but we all know these pathologies go beyond just tennis players. Construction workers, painters, and landscapers, to name a few are all subjected to elbow stresses due to the overuse of the wrist extensors with the gripping of various objects.
Prevention is the Key
Eccentric strengthening and selection of the proper grip-size of the objects being used is important. Optimal circumference of a device handle should equal the distance from the proximal palmar crease to the tip of the ring finger. This measurement assures the appropriate length-tension relationship for the finger flexors and wrist extensors to reduce the stress on the biarticulate muscles and thie attachment(s).
However, injury does occur on a rather frequent basis and often joint mobilization techniques are employed to assist in the recovery. Paungmail et al (2003) randomized 24 patients with lateral epicondylitis into three groups (mobilization, placebo, and control). Outcome measures were painfree grip strength (PFGS), pressure pain threshold (PPT), and thermal pressure threshold (TPT). The researchers delivered a lateral glide to the humeroulnar joint was situated just distal to the elbow joint line on the medial side of the ulna. The glide was applied and sustained for ~ 6 seconds while the patient performed a gripping action. Ten repetitions of the treatment technique were applied, with ~15-second rest intervals between repetitions. Each patient received three treatments ~72 hours apart. The mobilization with movement treatment group demonstrated a significant improvement in all outcome measures compared to the control and placebo groups. Bisset et al (2006) also examined the impact of mobilization with movement (MWM) compared to cortisone injection and control. The success rate for the MWM exceeded that of the comparison groups.
Mobilization Techniques
Let’s look at the mobilization techniques for the elbow: humero-ulnar medial glide for elbow flexion, humero-ulnar lateral glide to facilitate elbow extension, humero-radial anterior glide for flexion and pronation, and humero-radial posterior glide for extension in supination.
Elbow Flexion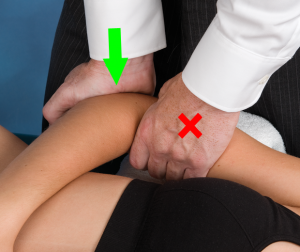
To perform a medial humero-ulnar glide to facilitate elbow flexion, the patient in the supine position. The arm is at the side and the elbow is flexed at 90 degrees. We typically allow the forearm to be draped across the anterior abdomen and a bolster or towel roll is placed under the distal humerus. The clinician will stand on the ipsilateral side, will stabilize the distal humerus and place the thenar eminence of the other hand over the olecranon and proximal ulna. Translation medially is used to improve elbow flexion.
 Elbow Extension
Elbow Extension
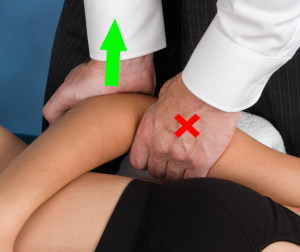
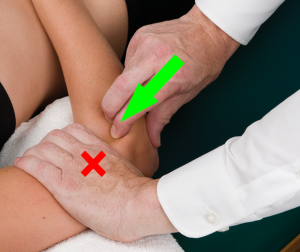
For a lateral glide, to facilitate extension, the patient is also in a supine position. The difference between a medial and lateral glide is a pushing versus a pulling motion, respectfully. The clinician pulls upward with lumbrical grip, i.e. the thenar eminence placed posterior over the olecranon and proximal ulna. Please note the orientation of the clinician’s forearm is parallel to the direction of movement in both techniques.
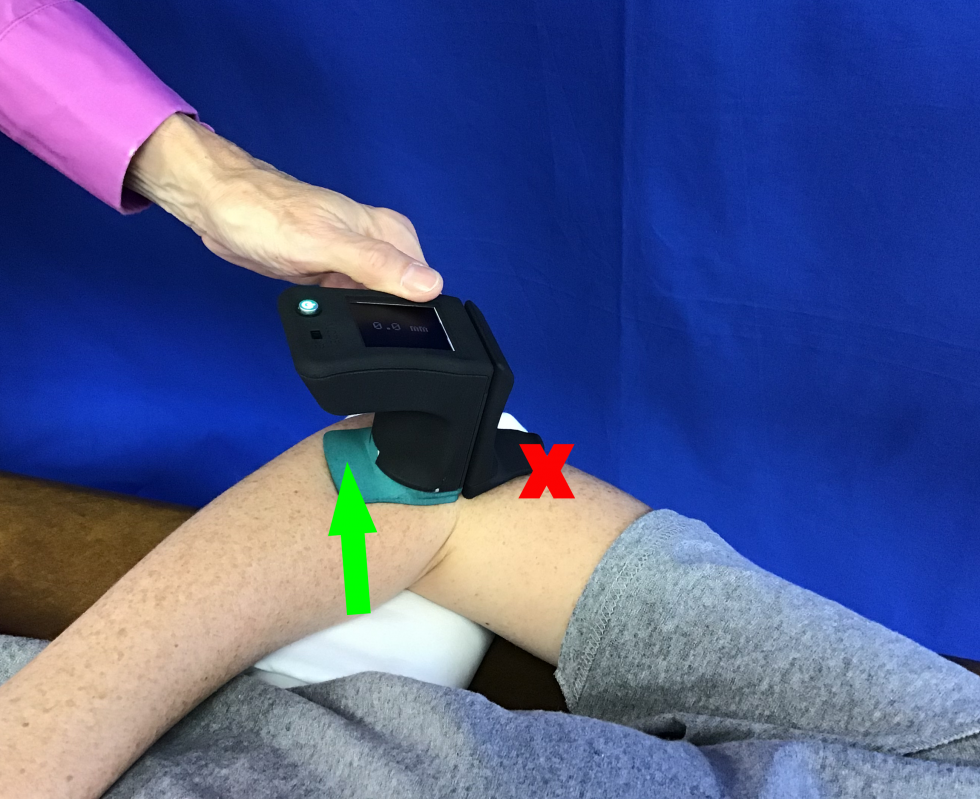
The Mobil–Aider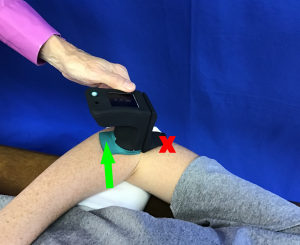
Quantifying the mobility of these techniques in millimeters of linear translation can be valuable. The process is exactly the same as the task described above. With the green (H-E) attachment, the Mobil–Aider can be used for medial and lateral glides. Given very limited magnitudes of movement with these techniques, the Mobil-Aider can be helpful in identifying differences between extremities and delivering consistent treatments.
 Pronation-Supination
Pronation-Supination
Other mobilization techniques for the elbow are humero-radial glides. These are performed in an anterior and posterior direction to facilitate flexion/pronation and extension/supination, respectfully. For both techniques the patient is in supine with the humerus is supported on a towel and the hand draped across the abdomen. The clinician stabilizes that humerus and grasps the proximal radius in three-jaw chuck pinch contact. The radius can be translated either anterior or posterior, depending on the movement to be facilitated. Figure 4 displays an anterior translation for flexion and pronation. Videos of the performance of these mobilization techniques can be viewed in the video learning modules of https://mobil-aider.com/
For more information on the Mobil-Aider device and joint mobilizations, please visit https://mobil-aider.com/
- Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: Randomised trial. British Medical Journal. 2006;333(7575):939.
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC, 2020
- Paungmali A, O’Leary S, Souvlis T, Vicenzino B. Hypoalgesia and sympathoexcitatoty effect of mobilization with movement for lateral epicondylitis. Physical Therapy. 2003;83:374-383
- Wise CH, Gulick DT. Mobilization Notes. FA Davis Publishing, Philadelphia, 2009