 When Convex-Concave Rule Meets Clinical Practice
When Convex-Concave Rule Meets Clinical Practice
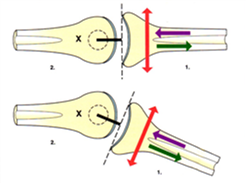
The convex-concave rule was developed by Freddie Kaltenborn. It has been taught for decades as the way to explain the arthrokinematics of a joint. It identifies that when the concave joint surface moves on the convex surface, rolling and gliding of the two surfaces occur in the same direction. Thus, if the concave joint surface rolls posterior, it will also glide posterior. However, if the convex joint surface moves on the concave surface, rolling and gliding occur in the opposite direction, i.e. if the convex surface rolls posterior, it will glide anterior on the concave surface. 
Simple right? Well, several researchers have questioned if the rule applies to clinical practice. This can be challenging to assess since we are talking about millimeters of motion. Until recently when the Mobil-Aider Arthrometer was developed to assess linear translation of 14 motions across five different joints (shoulder, elbow, wrist, knee, & ankle), arthrokinematics could not be objectively measured. More information about the Mobil-Aider, as well as the supporting research can be found at….. https://mobil-aider.com/
But let’s explore the concave-convex rule relative to clinical practice. Shoulder internal (IR) and external (ER) rotation is a good place to start. Based on the convex-concave rule, ER should be accompanied by rolling poste rior and gliding anterior. In other words, the convex humerus rolls posterior and glides anterior on the concave glenoid fossa. However, a study by Johnson et al (2007) compared the impact of both an anterior glide and a posterior glide of the shoulder on ER range of motion (ROM). The results demonstrated a 31 degree increase in ER ROM with a posterior glide as compared to just a 3 degrees increase with anterior glides. So how does that make sense? An anterior glide should occur with ER.
rior and gliding anterior. In other words, the convex humerus rolls posterior and glides anterior on the concave glenoid fossa. However, a study by Johnson et al (2007) compared the impact of both an anterior glide and a posterior glide of the shoulder on ER range of motion (ROM). The results demonstrated a 31 degree increase in ER ROM with a posterior glide as compared to just a 3 degrees increase with anterior glides. So how does that make sense? An anterior glide should occur with ER.
Sigel (2020) questioned if ER arthrokinematics involved spinning instead of rolling and gliding. Although capsular tightness was not assessed in the study, Neumann (2012) suggested the efficacy of the posterior glide could be related to capsular tightness. This tightness would skew the humeral head anterior and limit the amount of anterior translation available. A posterior glide could centralize the humeral head in the glenoid fossa. This centralization could unload the anterior capsule to provide more linear translation in the anterior direction for more ER. This research demonstrates the strong relationship between arthrokinematics and osteokinematics.
The take home message is the convex-concave rule is a wonderful guiding principle but the assessment of the joint limitation is paramount. Neumann states we “should not mobilize a pathological joint according to a rule, but treat pathological clinical findings, which are in correlation with the patient’s complaints.” In assessing posterior capsular restrictions of the shoulder, we must be sure to perform the technique correctly. Reinold (2015) discussed the importance of knowing anatomy of the shoulder and  appreciating the need to angle the posterior glide laterally to avoid hitting the posterior glenoid rim. Performing a posterior glide in the sagittal plane (not angled) could result in one thinking the glenoid rim endfeel is posterior capsule tightness. This would be a false representation of the arthrokinematics. Care should be taken to mobilize a joint with respect to the anatomic orientation.
appreciating the need to angle the posterior glide laterally to avoid hitting the posterior glenoid rim. Performing a posterior glide in the sagittal plane (not angled) could result in one thinking the glenoid rim endfeel is posterior capsule tightness. This would be a false representation of the arthrokinematics. Care should be taken to mobilize a joint with respect to the anatomic orientation.
In summary, the convex-concave rule has merit and is a good starting point. A thorough assessment of arthrokinematics and osteokinematics are prudent to determine the course of intervention.
If you would like to learn more about how the Mobil-Aider orthopedic measurement device can help you to quantify joint mobility, please visit: https://mobil-aider.com/
For more cutting-edge orthopedic information on orthopedic test and manual techniques, subscribe to iOrtho+ PREMIUM Web-based App at https://iortho.xyz/
- Baeyens JP, Van Roy P, Clarys JP. Intra-articular kinematics of the normal glenohumeral joint in the late preparatory phase of throwing: Kaltenborn’s rule revisited. Ergonomics. 2000 Oct;43(10):1726-1737
- Baeyens JP, Van Glabbeek F, Goossens M, Gielen J, Van Roy P, Clarys JP. In vivo 3D arthrokinematics of the proximal and distal radioulnar joints during active pronationand supination. Clinical Biomechanics. 2006 Jan;21:S9-12
- Gulick DT. iOrtho+ Premium Mobile App. DTG Enterprises LLC. 2021
- Johnson AJ, Godges JJ, Zimmerman GJ, Ounanian LL. The effect of anterior versus posterior glide joint mobilization on external rotation range of motion in patients with shoulder adhesive capsulitis. 2007 Mar;37(3):88-99
- Neumannn DA. The convex-concave rules of arthrokinematics: flawed or perhaps just misinterpreted?
- Reinold M. http://www.mikereinold.com/2015/10/how-to-assess-for-a-tight-posterior-capsule-of-the-shoulder.html
- Scarvell JM, Hribar N, Galvin CR, Pickering MR, Perriman DM, Lynch JT, Smith PN. Analysis of kneeling by medical imaging shows the femur moves back to the posterior rim of the tibial plateau, prompting review of the concave-convex rule. Physical Therapy. 2019 Mar;99(3):311-318
- Schomacher J. The convex-concave rule and the lever law. Manual Therapy. 2009 Oct;14(5):579
- Sigel K. https://www.physiotutors.com/kaltenborns-concave-convex-rule-flawed-or-just-misinterpreted/ Posted on July 25, 2020
- Wise CH, Gulick, DT. Mobilization Notes, FA Davis Publishing, Philadelphia.