
![]() Wrist Triangular FibroCartilage Complex
Wrist Triangular FibroCartilage Complex
The Triangular FibroCartilage Complex (TFCC) is an important structure in the wrist. It is a tough fibrous tissue that occupies the gap between the ulna and the proximal row of carpals. The function is to provide stability and cushion while transmitting an axial load between the carpals and the ulna. A FOOSH, a twisting motion (like a drill bit catching), and a radial fracture can result in tears of the TFCC. Tears tend to be more common with aging but individuals with a longer ulna may have a thinner TFCC and have a greater likelihood to tear. Although the TFCC blood supply comes from three sources: ulnar artery and palmar and dorsal branches of the interosseous artery, collectively the arteries only supply 15-20% of the periphery. The central region and the radial attachment of the TFCC are avascular. This anatomic orientation leads to very poor healing properties.
Signs and symptoms of an injured TFCC may include pain, clicking with wrist/forearm motion, and wrist/hand weakness. There are 3 TFCC tests: load test, press test, and GRIT. All of the tests utilize compression and/or ulnar deviation to “trap” the cartilage.
Load Test
The TFCC load test begins with the wrist in ulnar deviation. A longitudinal load is then applied through the 4th and 5th rays to the TFCC. A positive test is pain at the TFCC. One should remember, this position is similar to the clamp test for the scaphoid. Thus, being very distinct about the location of the pain could be important in distinguishing TFCC (ulnar joint line) pain versus scaphoid (anatomic snuffbox) pain.
Press Test
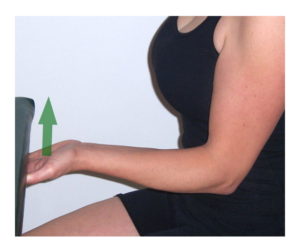
 The TFCC Press Test has been reported to be performed in two different ways. Those two techniques will be explained as Press Test #1 (left) and Press Test #2 (right). The first technique involves pressing the hand on the underside of a table or any immoveable object. The patient “presses up” like he/she is attempting to lift the table. This isometric contraction creates a load on the TFCC and can reproduce medial wrist pain. The second technique uses the upper extremities to “press up” from a chair. The closed chain position on the arms results in loading of the TFCC. Again, a positive test is medial wrist joint line pain.
The TFCC Press Test has been reported to be performed in two different ways. Those two techniques will be explained as Press Test #1 (left) and Press Test #2 (right). The first technique involves pressing the hand on the underside of a table or any immoveable object. The patient “presses up” like he/she is attempting to lift the table. This isometric contraction creates a load on the TFCC and can reproduce medial wrist pain. The second technique uses the upper extremities to “press up” from a chair. The closed chain position on the arms results in loading of the TFCC. Again, a positive test is medial wrist joint line pain.
GRIT Test

Another test that indirectly assesses and may incriminate the TFCC is the GRIT test. “GRIT” stands for Gripping Rotatory Impaction Test. Under normal circumstances, the act of gripping is accompanied by wrist extension with ulnar deviation. This combination of motions results in compression of the TFCC. Testing maximal grip strength can shed light on the health of the TFCC. Typically, we would expect to see that supination and pronation grip strength are equitable (ratio 1:1). LaStayo and Weiss (2001) and DeSmet (2005) looked at the GRIT with the idea that there may be a difference in supination versus pronation grip in TFCC injuries. When the elbow is supported in extension, grip strength has been reported to have the highest validity and reliability (Espana-Romero et al, 2010). So, in elbow extension, a hand-held dynamometer is placed in the client’s hand. Grip strength is assessed in both forearm pronation and supination. If the supinated grip exceeds the pronated grip (ratio > 1), an impaction of the TFCC is suggested.
If a hand-held dynamometer is not available, one can very easily do this test with a blood pressure cuff. You can pump up the blood pressure cuff to approximately 20 millimeters of mercury, have the patient grasp the inflated cuff and squeeze. The pressure on the dial will increase and then it is a simple math calculation, the delta = measurement minus your starting value of 20. This technique is performed in both supination and pronation.
This value can be important when an individual has chronic compression on the TFCC between the ulnar head and the proximal carpals. Ulnar impaction syndrome can lead to degenerative tearing of the TFCC and chondromalacia of the lunate, triquetrum, and distal ulnar head.
A simple pearl for the GRIT Impaction Ratio is:
TFCC Statistics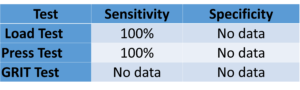
Data indicate they should only be used to screen out the presence of an TFCC injury. Mechanism of injury and clinical signs and symptoms may carry more weight in the diagnosis.
For videos on all of these tests and more cutting edge orthopedic information in iOrtho+ Premium Mobile App, please visit https://iortho.xyz/
- De Smet L. Magnetic resonance imaging for diagnosing lesions of the triangular fibrocartilage complex. Acta Orthop Belg. 2005;71(4):396-398.
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC, 2025
- Gulick, DT. OrthoNotes, 5th FA Davis Publishing, Philadelphia, 2023
- La Stayo P, Howell J. Clinical provocative tests used in evaluating wrist pain: a descriptive study. Journal Hand Therapy. 1995;8:10-17
- LaStayo P, Weiss S. The GRIT: a quantitative measure of ulnar impaction syndrome. Journal Hand Therapy. 2001;14(3):173-179.
- Lester B, et al. Press test for office diagnosis of triangular fibrocartilage complex tears of the wrist. Annals Plastic Surgery. 1995;35:41-45