

Quantifying ACL Testing
 The Anterior Cruciate Ligament (ACL) accounts for over a quarter million injuries per year, and that doesn’t count the number of re-injuries. In addition to identifying the mechanism of injury and symptoms such as popping or audible sound, immediate swelling, and instability in weight bearing, clinical tests are very important. These tests include the Lachman, anterior drawer, and Lelli test. In spite of the presence of a variety of tests, 74% of acute ACL injuries are misdiagnosed in the emergency department. For decades, the classic Lachman’s test has been considered the gold standard. It involves again translating the tibia on the femur. With the knee in ~20° of flexion, the distal portion of the femur is stabilized proximal to the knee and the tibia is translated anteriorly. However, there are some problems with the performance of the Lachman test….3 problems to be exact.
The Anterior Cruciate Ligament (ACL) accounts for over a quarter million injuries per year, and that doesn’t count the number of re-injuries. In addition to identifying the mechanism of injury and symptoms such as popping or audible sound, immediate swelling, and instability in weight bearing, clinical tests are very important. These tests include the Lachman, anterior drawer, and Lelli test. In spite of the presence of a variety of tests, 74% of acute ACL injuries are misdiagnosed in the emergency department. For decades, the classic Lachman’s test has been considered the gold standard. It involves again translating the tibia on the femur. With the knee in ~20° of flexion, the distal portion of the femur is stabilized proximal to the knee and the tibia is translated anteriorly. However, there are some problems with the performance of the Lachman test….3 problems to be exact.
- Protective muscle guarding of the hamstrings can restrict that anterior translation.
- Too much knee flexion can cause the posterior horn of the meniscus to act as a wedge and prevent translation of the tibia.
- There is often a mismatch between the size of the clinician’s hands and that of the patient’s leg circumference. Most clinicians have a hand span of somewhere in the vicinity of six to nine inches. Yet a lot of individuals who suffer ACL injuries will have thigh circumferences that exceed 18 to 23 inches. That creates a significant problem in being able to stabilize proximally with enough force to be able to generate a linear translation of the distal segment.
The Mobil–Aider Device
 Designed to address all of these pain points as well as provide a quantitative value on the linear translation of the knee, use of the Mobil–Aider device for the Lachman test is displayed. The contoured attachments distribute the contact forces over the anterior surfaces and the straps help to stabilize the device on any size knee. The bolster positions the knee in ~20° of flexion. The device is aligned with the joint line of the knee, the proximal segment is stabilized, and the distal segment is translated anteriorly. With the translation, the magnitude of the motion is displayed on the digital screen. Comparison with radiographs revealed a 6.9mm anterior translation with a reading of 7.1mm on the Mobil–Aider. That is less than a 2% margin of error in the testing of the device. These data is available here.
Designed to address all of these pain points as well as provide a quantitative value on the linear translation of the knee, use of the Mobil–Aider device for the Lachman test is displayed. The contoured attachments distribute the contact forces over the anterior surfaces and the straps help to stabilize the device on any size knee. The bolster positions the knee in ~20° of flexion. The device is aligned with the joint line of the knee, the proximal segment is stabilized, and the distal segment is translated anteriorly. With the translation, the magnitude of the motion is displayed on the digital screen. Comparison with radiographs revealed a 6.9mm anterior translation with a reading of 7.1mm on the Mobil–Aider. That is less than a 2% margin of error in the testing of the device. These data is available here.
Prone Lachman Test
Performing ACL testing in the prone position can allow gravity to be of assistance in anterior translation and stabilizing the thigh it not a challenging. For those of us with smaller hands and less than desirable upper body strength, this technique can offer an excellent alternate to the classic Lachman. Once in prone with the knee off the edge of the plinth and the lower leg supported, there are three different ways to apply the anterior translation: one-hand, two-hand, and forearm.



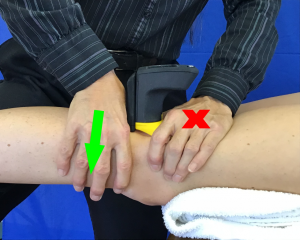 This position affords several advantages. As stated, gravity can assist with the motion. There are no issues with hand versus leg size. The likelihood of a false positive is decreased due to the elimination of tibial sag with a PCL injury. However, there is still no way to quantify millimeters of motion. By donning the yellow attachment on the Mobil–Aider, one can capitalize on all the advantages of the prone position and also quantify the magnitude of translation. So what is the criteria for a (+) Lachman test (classic or prone)? Quantitatively, a difference of 5 mm between involved and uninvolved knees is considered (+). Yet, there is also a qualitative component to the assessment. The ACL should abruptly stop the anterior translation of the tibia on the femur. If this does not occur, one should suspect an ACL injury.
This position affords several advantages. As stated, gravity can assist with the motion. There are no issues with hand versus leg size. The likelihood of a false positive is decreased due to the elimination of tibial sag with a PCL injury. However, there is still no way to quantify millimeters of motion. By donning the yellow attachment on the Mobil–Aider, one can capitalize on all the advantages of the prone position and also quantify the magnitude of translation. So what is the criteria for a (+) Lachman test (classic or prone)? Quantitatively, a difference of 5 mm between involved and uninvolved knees is considered (+). Yet, there is also a qualitative component to the assessment. The ACL should abruptly stop the anterior translation of the tibia on the femur. If this does not occur, one should suspect an ACL injury.
Anterior drawer test
 This is another ACL test that places the knee in 90° with the foot on the table. The clinician’s fingers are wrapped around the posterior knee to confirm the hamstrings are relaxed. The thumbs are placed on the anterior tibial plateau and the tibia is anteriorly translated on the femur. There are a number of causes of false negatives of the anterior drawer. This can include hemarthrosis and active synovitis that prevents putting the knee in the 90° test position, protective knee guarding of the hamstrings restricting anterior translation, and posterior horn medial meniscus wedging against the medial femoral condyle that can block anterior translation of the tibia. The advantage is the test is easy to perform regardless of hand and leg size.
This is another ACL test that places the knee in 90° with the foot on the table. The clinician’s fingers are wrapped around the posterior knee to confirm the hamstrings are relaxed. The thumbs are placed on the anterior tibial plateau and the tibia is anteriorly translated on the femur. There are a number of causes of false negatives of the anterior drawer. This can include hemarthrosis and active synovitis that prevents putting the knee in the 90° test position, protective knee guarding of the hamstrings restricting anterior translation, and posterior horn medial meniscus wedging against the medial femoral condyle that can block anterior translation of the tibia. The advantage is the test is easy to perform regardless of hand and leg size.
Lelli Test
 The test appeared in the literature in the last decade and uses a lever system to assess the integrity of the ACL. The patient is positioned in supine with the hip and knee extended. A foam roll is placed under the proximal third of the tibia. The clinician exerts a downward force to the distal third of the femur. With an intact ACL, the proximal tibia translates anterior, and as a result of the lever system, the foot then comes off the table. This is a negative test. If the ACL is not functioning, then a positive test would be the failure of the tibia to translate on the femur, and the heel of the involved leg would not rise off the table. Lelli et al (2014) reported 85% of ACL injuries are from the femoral attachment so it made more sense to manipulate the femur than the tibia. Although the metrics for this test are fairly good, it is still a binary test, either their positive or negative.
The test appeared in the literature in the last decade and uses a lever system to assess the integrity of the ACL. The patient is positioned in supine with the hip and knee extended. A foam roll is placed under the proximal third of the tibia. The clinician exerts a downward force to the distal third of the femur. With an intact ACL, the proximal tibia translates anterior, and as a result of the lever system, the foot then comes off the table. This is a negative test. If the ACL is not functioning, then a positive test would be the failure of the tibia to translate on the femur, and the heel of the involved leg would not rise off the table. Lelli et al (2014) reported 85% of ACL injuries are from the femoral attachment so it made more sense to manipulate the femur than the tibia. Although the metrics for this test are fairly good, it is still a binary test, either their positive or negative.
The statistical overview of the ACL tests is displayed below: 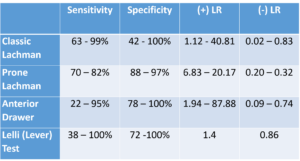
The clustering of the Lelli, pivot shift, anterior drawer, and Lachman has a 67% to 91% accuracy in the ACL diagnosis when all of these tests are (+). For more information on the Mobil–Aider and ACL testing, please download iOrtho+ Premium Mobile App or visit https://iortho.xyz/
Subscriptions are only $1.99/month or $9.99/year. Over 450 clinical tests and over 120 manual techniques available via this WEB app – accessible on any device.
FYI – Prior blog posts are available at https://iortho.xyz/
Information on the Mobil-Aider Arthrometer to quantify joint mobility can be found at https://iortho.xyz/
- Abruscato K, Browning K, Deleandro D, Menard Q, Wilhelm M, Hassen A. Diagnostic accuracy of the Lever sign in detecting ACL tear: A systematic review and meta-analysis. IJSPT. 2019 (Feb);12(1)
- Almonroeder TG, Kernozek T, Cobb S, Stevens B, Huddleston W. Cognitive demands influence lower extremity mechanics during a drop vertical jump task in female athletes. JOSPT. 2018;48(5):381-387
- Arneja A, Leith J. Review article: Validity of the KT-1000 knee ligament arthrometer. Journal of Orthopaedic Surgery. 2009;17(1):77-79
- Bach BR, Warren RF, Wickiewitz TL: The pivot shift phenomenon: results and description of a modified clinical test for anterior cruciate ligament insufficiency, American Journal Sports Medicine. 1988; 16:571-576
- Baker CL, Norwood LA, Hughston JC. Acute combined posterior cruciate & posterolateral instability of the knee. American Journal of Sports Medicine. 1984;12(3):204-208
- Benjaminse A, Gokeler A, van der Schans CP. Clinical diagnosis of an anterior cruciate ligament rupture: A meta-analysis. Journal Orthopedic & Sports Physical Therapy. 2006;36(5):267-288
- Boeree NR, Ackroyd CE. Assessment of the meniscus & cruciate ligaments: an audit of clinical practice. Injury. 1991;22(4):291-294
- Boyer P, Dijan P, Christel P, Paoletti X, Degeorges R. Reliability of the KT-1000 arthrometer (Medmetric) for measuring anterior knee laxity: comparison with Telos in 147 knees. Revue de chirurgie orthopedique et reparatrice de l’appareil moteur 2004;90(8):757-764
- Cibere J, Bellamy N, Thorne A, Esdaile JM, McGorm KJ, Chalmers A, et al. Reliability of the knee examination in osteoarthritis: effect of standardization. Arthritis Rheumatism. 2004;50:458-468
- Cooperman JM, Riddle DL, Rothstein JM: Reliability and validity of judgments of the integrity of the anterior cruciate ligament of the knee using the Lachman test, Physical Therapy 1990;70:225-233
- Daniel DM, Stone ML, Barnett P, Sachs R. Use of the quadriceps active test to diagnose posterior cruciate ligament disruption & measure posterior laxity of the knee. Journal of Bone & Joint Surgery. 1988;70:386-391
- De Lee JC: Ligamentous injury of the knee. In Stanitski CL, DeLee JC, Drez D, editors: Pediatric and adolescent sports medicine, Philadelphia, 1994, WB Saunders.
- Dervin GF, Stiell IG, Wells GA, et al. Physicians’ accuracy & inter-rater reliability for the diagnosis of unstable meniscal tears in patients having osteoarthritis of the knee. Canadian Journal Surgery. 2001;44:267-274
- Deveci A, Cankaya D, Yilmaz S, Ozdemir G, Arslantas E, Bozkurt M. The arthroscopical & radiological correlation of lever sign test for diagnosis of anterior cruciate ligament rupture. 2015;4:830
- Ekegren CL, Miller WC, Celebrini RG, Eng JJ, Macintyre DL. Reliabilty & validity of observational risk screening in evaluating dynamic knee valgus. Journal of Orthopedic & Sports Physical Therapy. 2009;39(9):665-674
- Ferrari DA, Ferrari JD, Coumas J: Posterolateral instability of the knee, Journal Bone Joint Surgery America 1994;76:187-192
- Fowler PJ, Messieh SS. Isolated posterior cruciate ligament injuries in athletes. American Journal Sports Medicine. 1987;15:553-557
- Frank C: Accurate interpretation of the Lachman test, Clinical Orthopedics 1986;213:163-166
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2025
- Gulick DT. OrthoNotes, 5th edition, FA Davis Publishing, Philadelphia. 2024
- Hardaker WT, Garrett WE, Bassett FH. Evaluation of acute traumatic hemarthrosis of the knee joint. Southern Medical Journal. 1990; 83(6):640-646
- Jain DK, Amaravati R, Sharma G. Evaluation of the clinical signs of anterior cruciate ligaments & meniscal injuries. Indian Journal of Orthopedics. 2009;43(4):375-378
- Jarbo KA, Hartigan DE, Scott KL, Patel KA, Chhabra A. Accuracy of the Lever sign test in the diagnosis of anterior cruciate ligament injuries. Orthopaedic Journal of Sports Medicine. 2017;5(10):1-7
- Jonsson T, Althoff B, Peterson L et al: Clinical diagnosis of ruptures of the anterior cruciate ligament: a comparative study of the Lachman test and the anterior drawer sign, American Journal Sports Medicine. 1982;10:100-102
- Katz J, Fingeroth R. The diagnostic accuracy of ruptures of the anterior cruciate ligament comparing the Lachman test, the anterior drawer sign, & the pivot shift test in acute & chronic knee injuries. American Journal Sports Medicine. 1986;14:88-91
- Khayambashi K, Ghoddosi N, Straub RK, Powers CM. Hip muscle strength predicts noncontact anterior cruciate ligament injury in male and female athletes: A prospective study. American Journal of Sports Medicine. 2016 Feb;44(2):355-361
- Lee JK, Yao L, Phelps CT, Wirth CR, Czajka J, Lozman J. Anterior cruciate ligament tears: MR imaging compared with arthroscopy & clinical tests. Radiology. 1988;166:861-864
- Lelli A, DiTuri RP, Spenciner DB, Domini M. The Lever Sign: A new clinical test for the diagnosis of anterior cruciate ligament rupture. Knee Surgery Sport Traumatology & Arthroscopy. 2014
- Lichtenberg MC, Koster CH, Teunissen LPJ, Oosterveld FGJ, Harmsen AMK, Haverkamp D, Hoornenborg D, Berg RP, Bloemers FW, Faber IR. Does the Lever Sign Test have added value for diagnosing anterior cruciate ligament ruptures? Orthopaedic journal of sports medicine 2018 Mar; 6(3): 232
- Logan MC, Williams A, Lavelle J et al: What really happens during the Lachman test: a dynamic MRI analysis of tibiofemoral motion, American Journal Sports Medicine. 2004;32:369-375
- Loos WC, Fox JM, Blazina ME, Del Pizzo W, Friedman MJ. Acute posterior cruciate ligament injuries. American Journal of Sports Medicine. 1981;8(2):86-92
- Losee RE, Ennis TRJ, Southwick WO: Anterior subluxation of the lateral tibial plateau: a diagnostic test and operative review, Journal Bone Joint Surgery American 1978;60:1015-1030
- Lui SH, Osti L, Henry M, Bocchi L. The diagnosis of acute complete tears of the anterior cruciate ligament. Journal of Bone & Joint Surgery. 1995;77:586-588
- Magee D. Orthopedic Physical Assessment. 5th ed. Philadelphia, PA: WB Saunders Company; 2008.
- Malanga GA, Andrus S, Nadler SF, McLean J. Physical examination of the knee: A review of the original test description & scientific validity of common orthopedic tests. Archives Physical Medicine Rehabilitation. 2003;84:592-603
- Mitsou A, Vallianatos P. Clinical diagnosis of ruptures of the anterior cruciate ligament: a comparison between the Lachman test & the anterior drawer test. Injury. 1988;19(6):427-428
- Muller W: The knee: form, function and ligament reconstruction, New York, 1983, Springer-Verlag.
- Mulligan EP, Anderson A, Watson S, Dimeff RJ. The diagnostic accuracy of the Lever Sign for detecting anterior cruciate ligament injury. International Journal of Sports Physical Therapy. 2017;12(7):1057-1067
- Mulligan EP, Harwell JL, Robertson WJ. Reliability & diagnostic accuracy of the Lachman test performed in a prone position. Journal Orthopedic & Sports Physical Therapy. 2011;41(10):749-757
- Ostrowski JA. Accuracy of 3 diagnostic tests for anterior cruciate ligament tears. Journal of Athletic Training. 2006;41(1):120-121
- Padua DA, DiStefano LJ, Beutier AI, de la Motta SJ, DiStefano MJ, Marshall SW. The Landing Error Scoring System as a screening tool for an anterior cruciate ligament injury- Prevention program in elite-youth soccer athletes. Journal of Athletic Training. 2015;50(6):589-595.
- Paessler HH, Michel D: How new is the Lachman test? American Journal Sports Medicine. 1992;20:95-98
- Peterson L, Pitman MI, Gold J: The active pivot shift: the role of the popliteus muscle, American Journal Sports Medicine. 1984;12:313-317
- Rebman LW: Lachman test: an alternative method, Journal Orthopedic & Sports Physical Therapy 1988;9:381-382
- Redler LH, Watling JP, Dennis ER, Swart EF, Ahmad CS, Physician and non-physician inter- and intra-observer reliability of a field-based drop vertical jump screening test for ACL injury risk. Orthopedic Journal of Sports Medicine. 2015 July ePub
- Reiman MP, Reiman CK, Decary S. Accuracy of the Lever sign to diagnose anterior cruciate ligament tear: A systematic review with meta-analysis. International Journal of Sports Physical Therapy. 2018;13(5):774-788
- Rosenberg TD, Rasmussen GL: The function of the anterior cruciate ligament during anterior drawer and Lachman testing, American Journal Sports Medicine 1984;12:318-322
- Rubinstein RA, Shelbourne KD, McCarroll JR, van Meter CD, Rettig AC. The accuracy of the clinical examination in the setting of posterior cruciate ligament injuries. American Journal of Sports Medicine. 1994;22:550-557
- Shelbourne KD, Benedict F, McCarroll JR et al: Dynamic posterior shift test: an adjuvant in evaluation of posterior tibial subluxation, American Journal Sports Medicine. 1989;17:275-277
- Shino K, Horibe S, Ono K: The voluntary evoked posterolateral drawer sign in the knee with posterolateral instability, Clinical Orthopedics 1987;215:179-186
- Staubi H-U, Jakob RP. Posterior instability of the knee near extension. Journal of Bone & Joint Surgery. 1990;72-B:225-230
- Strobel M, Stedtfeld HW: Diagnostic evaluation of the knee, Berlin, 1990, Springer-Verlag.
- Tonino AJ, Huy J, Schaafsma J. The diagnostic accuracy of knee testing in the acutely injured knee. ACTA Orthopedia. 1986;52(4):479-487
- Veltri DM, Warren RF: Isolated and combined posterior cruciate ligament injuries, J Am Acad Orthop Surg. 1993; 1:67-75
- Weatherwax RJ: Anterior drawer sign, Clin Orthop. 1981; 154:318-319
- Wise CH, Gulick DT. Mobilization Notes. FA Davis Publishing, Philadelphia. 2009
- Wood L, Peat G, Wilkie R, et al. A study of the noninstrumental physical examination of the knee found high observer variability. Journal of Clinical Epidemiology. 2006;59:512-520