Not All Ankle Sprains Are Equal


Ankle Sprain Mechanisms
Injuries to ankle ligaments typically fall into one of two buckets. Lateral ankle sprains are the result of an inversion with plantarflexion stress and syndesmotic, AKA high ankle sprains, are attributed to forceful dorsiflexion with eversion. Approximately 85% of ankle sprains injure the lateral ligaments. This is primarily due to the more distal projection of the lateral malleolus and the very strong deltoid ligament. Of the lateral ligaments, 60-70% of the injuries are to the anterior talofibular (ATF) ligament, 20% involve to ATF and calcaneofibular (CF), and 14% are avulsion injuries.
Ankle Sprain Symptom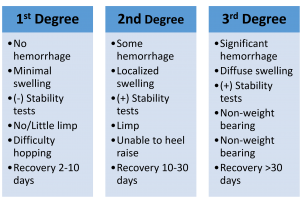
Symptoms include edema, pain, ecchymosis, and possibility instability. The magnitude of the symptoms are used to classify the sprain as grade I, II, or III. The chart below summarizes the grades:
Ankle Functional Questionnaires
In addition to the clinical signs and symptoms, there are a variety of clinical questionnaires to help the clinician appreciate the functional limitations of a patient with an ankle injury. Here are a few:
- Cumberland Ankle Instability Tool (CAIT) http://www.archives-pmr.org/article/S0003-9993(06)00519-3/pdf
- Foot & Ankle Ability Measure (FAAM) https://www.sralab.org/sites/default/files/2017-06/Foot%20and%20Ankle%20Ability%20Measure.pdf
- Foot & Ankle Disability Index (FADI) Score https://www5.aaos.org/uploadedFiles/foot_and_ankle_disab.pdf
Lateral Ankle Sprain Tests
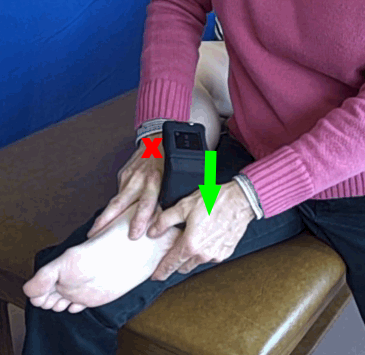
To test the lateral ligaments, the anterior drawer and talar tilt are the primary tests. The anterior drawer test stresses for ATF to determine laxity. The ATF connects the tibia and the fibula so displacing the calcaneus anterior on the stabilized tibia-fibula will incriminate this ligament. To perform this test, the patient is in supine with the distal tibia/fibula stabilized and the posterior calcaneus/talus grasped to translate anterior on tibia/fibula, i.e. distal moved on proximal. A positive test is pain and/or excessive gapping. You should also note, the presence of a “dimple” anterior to the tip of the lateral malleous during the drawer test is a positive indication of an ATF ligament rupture. This “dimple” is the result of negative pressure created by anterior displacement of the talus drawing the skin inward.
A study by Kovaleski et al (2008) examined the influence of knee and ankle position on anterior ankle laxity. Stiffness was determined to be greatest at 0° of knee and ankle flexion. Laxity was maximal at 90° of knee flexion with 10° of plantarflexion. Therefore, if testing is performed in a position of maximal stiffness and laxity is determined to be present, it can be attributed to ankle capsuloligamentous structures.
A recent study that examined the use of the Mobil–Aider Arthrometer reported a 1.1 mm difference between the injured and uninjured ankles was consistent with a grade I ankle sprain and a difference of 2.2 mm was consistent with a grade II ankle sprain. This quantitative information is critical in driving the plan for interventions (Taweel, Gulick, Palombaro, 2022).
difference between the injured and uninjured ankles was consistent with a grade I ankle sprain and a difference of 2.2 mm was consistent with a grade II ankle sprain. This quantitative information is critical in driving the plan for interventions (Taweel, Gulick, Palombaro, 2022).
 The talar tilt test has three alternatives to enable the clinician to implicate any one of three ligaments: ATF, CF, posterior talofibular (PTF). In order to do this, the clinician stabilizes the lower leg and grasps the calcaneus to apply a varus stress. The position of the ankle determines the primary ligament stressed: plantarflexion = ATF, neutral = CF, and dorsiflexion = PTF.
The talar tilt test has three alternatives to enable the clinician to implicate any one of three ligaments: ATF, CF, posterior talofibular (PTF). In order to do this, the clinician stabilizes the lower leg and grasps the calcaneus to apply a varus stress. The position of the ankle determines the primary ligament stressed: plantarflexion = ATF, neutral = CF, and dorsiflexion = PTF. 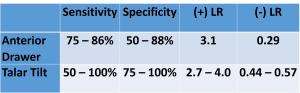 That is not to say the other ligaments are not stressed in the respective positions but it would not be the ligament of maximal stress. A positive test is pain and/or excessive gapping. The statistical values for these tests demonstrate the confidence by which they should be interpreted.
That is not to say the other ligaments are not stressed in the respective positions but it would not be the ligament of maximal stress. A positive test is pain and/or excessive gapping. The statistical values for these tests demonstrate the confidence by which they should be interpreted.
Syndesmotic Ankle Sprain Tests
 The syndesmotic tests include the squeeze, external rotation, cotton, and fibular translation tests. A syndesmotic sprain is one in which the ankle mortise, the junction of the tibia and fibula, is separated. This occurs with forceful dorsiflexion as the wider base of the trapezoidal shaped talus forces the tibia and fibula apart. The syndesmotic squeeze test can be performed in supine or sitting. It begins at the proximal tibia/fibula and the clinician begins squeezing the tibia/fibula together proximally and progresses distally towards the ankle until pain is felt. The squeezing motion will gap the syndesmosis and the farther from the ankle that pain is elicited, the more severe the sprain. Care must be taking to squeeze the tibia/fibula and not anterior/posterior soft tissue. This is not meant to be a Homan sign for DVTs.
The syndesmotic tests include the squeeze, external rotation, cotton, and fibular translation tests. A syndesmotic sprain is one in which the ankle mortise, the junction of the tibia and fibula, is separated. This occurs with forceful dorsiflexion as the wider base of the trapezoidal shaped talus forces the tibia and fibula apart. The syndesmotic squeeze test can be performed in supine or sitting. It begins at the proximal tibia/fibula and the clinician begins squeezing the tibia/fibula together proximally and progresses distally towards the ankle until pain is felt. The squeezing motion will gap the syndesmosis and the farther from the ankle that pain is elicited, the more severe the sprain. Care must be taking to squeeze the tibia/fibula and not anterior/posterior soft tissue. This is not meant to be a Homan sign for DVTs.
 The external rotation test (AKA Kleiger test) is performed in supine with the knee flexed to 90°. The clinician uses one hand to support the lower leg. The other hand supports the talocrural joint in neutral and imparts an ER force to the ankle to displace the fibula laterally to open up the mortise. Reproduction of pain is a positive test.
The external rotation test (AKA Kleiger test) is performed in supine with the knee flexed to 90°. The clinician uses one hand to support the lower leg. The other hand supports the talocrural joint in neutral and imparts an ER force to the ankle to displace the fibula laterally to open up the mortise. Reproduction of pain is a positive test.
 The Cotton (Shunk) test utilizes a lateral translation against the fibula to separate the mortise. In supine or sitting, the clinician stabilizes the distal tibia and grasps the rearfoot with the other hand. Note the rearf
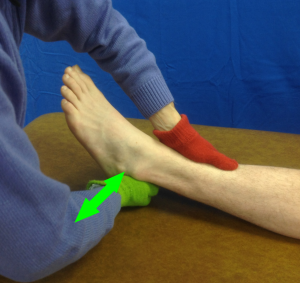
The Cotton (Shunk) test utilizes a lateral translation against the fibula to separate the mortise. In supine or sitting, the clinician stabilizes the distal tibia and grasps the rearfoot with the other hand. Note the rearf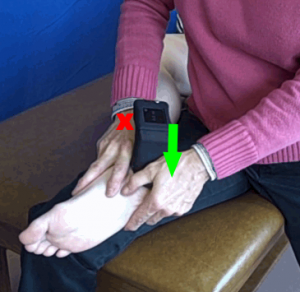 oot is translated medial and lateral. This is not an inversion and eversion motion to produce gapping. A positive test is translation in either direction of more than 3-5 mm or the presence of a “clunk.” Assessment of millimeters of translation is challenging. The Mobil–Aider device can provide this data.
oot is translated medial and lateral. This is not an inversion and eversion motion to produce gapping. A positive test is translation in either direction of more than 3-5 mm or the presence of a “clunk.” Assessment of millimeters of translation is challenging. The Mobil–Aider device can provide this data.
 The fibular translation test places the client in contralateral sidelying for the clinician to apply an anterior-posterior force (sagittal plane) to the distal fibula. Increased translation as compared to the contralateral side would be a positive test.
The fibular translation test places the client in contralateral sidelying for the clinician to apply an anterior-posterior force (sagittal plane) to the distal fibula. Increased translation as compared to the contralateral side would be a positive test.
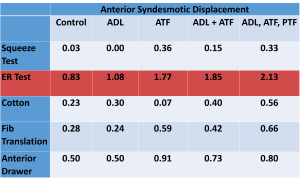
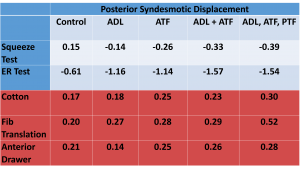
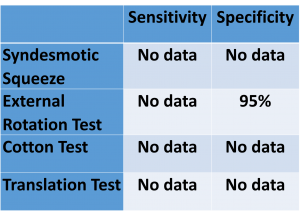 Aside from the external rotation test, there is no sensitivity or specificity reported for the syndesmotic tests. However, a study conducted by Beumer et al (2003) looked at the different tests for the syndesmotic ankle instability, with the purpose of determining the best tests to identify laxity. With the systematic sectioning of precise ligaments, they looked at the squeeze, the fibular translation, the cotton, the external rotation, and the anterior drawer. The charts below summarize the data for anterior and posterior displacement of the syndesmosis. Data reveals the External Rotation Test produces the most anterior gapping while the Cotton, Fibular Translation, and Anterior Drawer tests produce similar magnitudes of posterior gapping.
Aside from the external rotation test, there is no sensitivity or specificity reported for the syndesmotic tests. However, a study conducted by Beumer et al (2003) looked at the different tests for the syndesmotic ankle instability, with the purpose of determining the best tests to identify laxity. With the systematic sectioning of precise ligaments, they looked at the squeeze, the fibular translation, the cotton, the external rotation, and the anterior drawer. The charts below summarize the data for anterior and posterior displacement of the syndesmosis. Data reveals the External Rotation Test produces the most anterior gapping while the Cotton, Fibular Translation, and Anterior Drawer tests produce similar magnitudes of posterior gapping.
In summary, a positive test of all ankle ligamentous tests is pain and/or increased translation of the joint. It is always helpful to make a contralateral comparison if the other ankle is healthy. For more cutting edge orthopedic information in iOrtho+ Premium Mobile App, please visit https://iortho.xyz/
For more information on the Mobil–Aider Arthrometer, please visit: https://mobil-aider.com/
- Alonso A, Khoury L, Adams R: Clinical tests for ankle syndesmosis injury: reliability and prediction of return to function, Journal Orthopedic & Sports Physical Therapy 1998;27:276-284
- Aradi AJ, Wong J, Walsh M: The dimple sign of a ruptured lateral ligament of the ankle: brief report, Journal Bone Joint Surgery British 1988;70:327-328
- Baumhauer JF, Alosa DM, Renstrom AF, Trevino S, Beynnon B. A prospective study of ankle injury risk factors. American Journal of Sports Medicine. 1995;23(5): 564-570
- Beumer A, Swierstra BA, Mulder PG. Clinical diagnosis of syndesmotic ankle instability: evaluation of stress tests behind the curtains. Acta Orthopedics Scandanavia. 2002;73(6):667-669
- Beumer A, van Hemert WL, Swierstra BA, Jasper LE, Belkoff SM. A biomechanical evaluation of clinical stress tests for syndesmotic ankle instability. Foot Ankle International. 2003;24(4):358-363
- Birrer RB, Cartwright TJ, Denton JR: Immediate diagnosis of ankle trauma, Physician Sport Medicine 1994;22:95-102
- Boytim MJ, Fischer DA, Neuman L: Syndesmotic ankle sprains, American Journal Sports Medicine 1991;19:294-298
- Brosky T, Nyland J, Nitz A et al: The ankle ligaments: consideration of syndesmotic injury and implications for rehabilitation, Journal Orthopedic & Sports Physical Therapy 1995;21:197-205
- Candal-Couto JJ, Burrow D, Bromage S, Briggs PJ. Instability of the tibio-fibular syndesmosis: have we been pulling in the wrong direction? 2004;35(8):814-818
- Colter JM: Lateral ligamentous injuries of the ankle. In Hamilton WC, editor: Traumatic Disorders of the Ankle, New York, 1984, Springer-Verlag
- Cotton FJ: Fractures and fracture-dislocations, Philadelphia, 1910, WB Saunders.
- Davidovitch RI, Weil Y, Karia R, Forman J, Looze C, Liebergall M, Egol K. Intraoperative syndesmotic reduction: three-dimensional versus standard fluoroscopic imaging. Journal of Bone and Joint Surgery. 2013;95(20):1838-1843
- Dutton M, Orthopaedic Examination, Evaluation, & Intervention: A Pocket Handbook. NY: McGraw-Hill, 2005
- Frost HM, Hanson CA: Technique for testing the drawer sign in the ankle, Clinical Orthopedics 1977;123:49-51
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Gungor T: A test for ankle instability: brief report, J Bone Joint Surg Br. 1988; 70:487
- Hertel J, Denegar CR, Monroe MM, Stokes WL. Talocrural & subtalar joint instability after lateral ankle sprain. Medicine Science Sports Exercise. 1999;31:1501-1508
- Hollis JM, Blasier RD, Flahiff CM: Simulated ankle ligamentous injury: change in ankle stability, Am J Sports Med. 1995; 23:672-677
- Hopkinson WJ, St Pierre P, Ryan JB et al: Syndesmosis sprains of the ankle, Foot Ankle 1990;10:325-330
- Kjaersgaard-Andersen P, Frich LH, Madsen F et al: Instability of the hindfoot after lesion of the lateral ankle ligaments: investigations of the anterior drawer and adduction maneuvers in autopsy specimens, Clinical Orthopedics 1991;266:170-179
- Kovaleski JE, Norrell PM, Heitman RJ, Hollis JM, Pearsall AW. Knee and ankle position, anterior drawer laxity, and stiffness of ankle complex. Journal of Athletic Training. 2008 May-June;43(3):242-248
- Lin C-F, Gross MT, Weinfeld P: Ankle syndesmosis injuries: anatomy, biomechanics, mechanism of injury, and clinical guidelines for diagnosis and intervention, Journal Orthopedic & Sports Physical Therapy. 2006;36:372-384
- Lindstrand A: New aspects in the diagnosis of lateral ankle sprains, Orthopedic Clinics North America 1976;7:247-249
- Martin RL, Davenport TE, Paulseth S, Wukich DK, Godges JJ. Ankle Stability and Movement Coordination Impairments: Ankle Ligament Sprains. JOSPT. 2013;43(9):1-40.
- Mizel MS. Technique tip: a revised method of the Cotton test for intra-operative evaluation of syndesmotic injuries. Foot Ankle International. 2003;24(1):86-87
- Norkus SA, Floyd RT: The anatomy and mechanisms of syndesmotic ankle sprains, Journal Athletic Training. 2001;36:68-73
- Nussbaum ED, Hosea TM, Sieler SD et al: Prospective evaluation of syndesmotic ankle sprains without diastasis, American Journal Sports Medicine 2001;29:31-35
- Peng JR: Solving the dilemma of the high ankle sprain in the athlete, Sports Medicine Arthroscopic Review. 2000;8:316-325
- Phisitkul P, Chaichankul C, Sripongsai R, Prasitdamrong I, Tengtrakulcharoen P, Suarchawaratana S. Accuracy of anterolateral drawer test in lateral ankle instability: A cadaveric study. Foot & Ankle International. 2009;30(7):690-695
- Raatikainen T, Putkonen M, Puranen J. Arthrography, clinical exami¬nation, and stress radiograph in the diagnosis of acute injury to the lateral ligaments of the ankle. Am J Sports Med. 1992;20:2-6
- Tawell NR, Gulick DT, Palombaro KM. Asessing lateral ankle sprains with a new arthrometer. 2022
- Tohyama H, Yasuda K, Ohkoshi Y et al: Anterior drawer test for acute anterior talofibular ligament injuries of the ankle: how much load should be applied during the test? American Journal Sports Medicine 2003;31:226-232
- Trojian TH, McKeag DB. Ankle sprains expedient assessment & management. Physician & Sports Medicine. 1998;26(10):29-40
- van den Bekerom MPJ. Diagnosing syndesmotic instability in ankle fractures. World Journal 2011;18;2(7):51-56
- van Dijk CN, Lim LS, Bossuyt PM, Marti RK. Physical examination is sufficient for the diagnosis of sprained ankles. J Bone Joint Surg Br. 1996;78:958-962.
- Williams GN, Allen EJ. Rehabilitation of Syndesmotic (High) Ankle Sprains. Sports Health. 2010; 2(6): 460-470
- Wright RW, Barile RJ, Surprenant DA et al: Ankle syndesmosis sprains in national hockey league players, American Journal Sports Medicine 2004;32:1941-1945