


Lower Limb Tension Tests : SLR Variations
Lower limb tension tests (LLTT), also known as neural tension tests, are used to evaluates the length and mobility of the components of the nervous system. This blog will discuss the 8 techniques of the lower extremity: sciatic, tibial, sural, common peroneal, femoral, lateral femoral cutaneous, obturator, and saphaneous nerves.
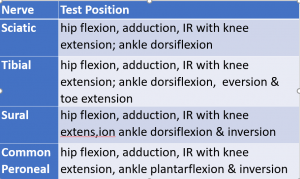
Testing of the sciatic nerve can be done via combinations of four different positions to incriminate the sciatic, tibial, sural, and common peroneal nerves. All sciatic nerve tests begin in the supine position and a straight leg raise (SLR) is performed, i.e. hip flexion, knee extension. Each of the tests would be deemed positive if the neurological symptoms are reproduced. The chart below distinguishes the defining characteristics for the testing of each the nerves:
Overall, SLR testing is highly variable. Statistically ranges as seem below are not clinically helpful.
- Sensitivity = 40-98%
- Specificity = 10-100%
- (+) Predictive value = 83%
- (-) Predictive value = 64%
- (+) Likelihood ratio = 1.0-1.98
- (-) Likelihood ratio = 0.05-0.86
- Reliability (Kappa) = 0.32-0.86



| Tibial | Sural | Common Peroneal |
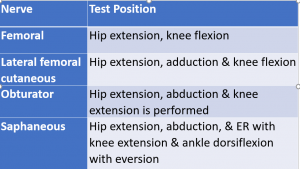
Prone knee bend testing allows for the assessment of the femoral, lateral femoral cutaneous, obturator, and saphenous nerves. All of these tests begin in the prone position. The chart below differentiates the various positions for each nerve:
A positive test is a reproduction of the neurological symptoms. Unfortunately, there is not any literature on sensitivity but specificity is very high (84%) while the reliability of testing is low (Kappa = 0.21-0.26).




| Femoral | Lateral Femoral Cutaneous | Obturator | Saphaneous |
Once determined there is a concern with the mobility of a nerve, the same positioning maneuvers can be used as treatment. This is called neural flossing. It is a gentle technique in which tension is briefly applied to the nerve in the specific position described. The tension is removed and reapplied for several repetitions, i.e. “pressure on, pressure off” for 10-15 repetitions. Paresthesia may be experienced during the “pressure on” phase but should diminish during the “pressure off” phase. The purpose of neural flossing is to free a nerve of adhesions and increase mobility.
![]() For videos of these techniques or more cutting-edge orthopedic information subscribe to iOrtho+ Premium Web App. To subscribe or access prior blog posts, please visit https://iortho.xyz/
For videos of these techniques or more cutting-edge orthopedic information subscribe to iOrtho+ Premium Web App. To subscribe or access prior blog posts, please visit https://iortho.xyz/
- Breig A, Troup JDG: Biomechanical considerations in straight-leg-raising test: cadaveric & clinical studies of the effects of medical hip rotation, Spine 1979;4:242-250
- Charnley J: Orthopedic signs in the diagnosis of disc protrusion with special reference to the straight-leg-raising test, Lancet 1951;1:186-192
- DeVille W, van der Windt D, Dzaferagic A, Bezemer P, Bouter L. The test of Lasegue Systemic review of the accuracy in diagnosing herniated discs. Spine. 2000;25:1140-1147
- Edgar MA, Park WM: Induced pain patterns on passive straight-leg-raising in lower lumbar disc protrusion, Journal Bone Joint Surgery British 1974;56:658-667
- Fahrni WH: Observations on straight-leg-raising with special reference to nerve root adhesions, Canadian Journal Surgery 1966;9:44-48
- Flynn T, Fritz J, Whitman J, et al. A clinical prediction rule for classifying patients with low back pain who demonstrated short-term improvement with spinal manipulation. Spine. 2002;27:2835-2843
- Goddard BS, JD Reid: Movements induced by straight-leg-raising in the lumbosacral roots, nerves, & plexus and in the intrapelvic section of the sciatic nerve, Journal Neurology Neurosurgery Psychiatry 1965;28:12-18
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Jonsson B, Stromqvist B. The straight leg raising test & the severity of symptoms in lumbar disc herniation. Spine. 1995;20:27-30
- Kosteljanetz M, Espersen J, Halaburt H, Miletec T. Predictive value of clinical & surgical findings in patients with lumbago-sciatica. Acta Neurochiropractic. 1984;73:67-76
- Kuo L, Chung W, Bates E, Stephen J: The hamstring index, Journal Pediatric Orthopedics 1997;17:78-88
- Majlesi J, Togay H, Unanlan H, Toprak S. The sensitivity & specificity of the slump & SLR tests in patients with lumbar disc herniation. Journal of Clinical Rheumatology. 2008;14(2):87-91
- Mens J, Vleeming A, Snijders C, Koes B, Stam H. Reliability & validity of the active straight leg raise test in posterior pelvic pain since pregnancy. Spine. 2003;26:1167-1171
- Postacchini F, Cinotti G, Gumina S: The knee flexion test: a new test for lumbosacral root tension, Journal Bone Joint Surgery British 1993;75:834-835
- Potter N, Rothstein J. Intertester reliability for selected clinical tests of the sacroiliac joint. Physical Therapy. 1985;65:1671-1675
- Riddle D, Freburger J. Evaluation of the presence of sacroiliac joint dysfunction using a combination of tests: a multicenter intertester reliability study. Physical Therapy. 2002;82:772-781
- Rose M. The statistical analysis of the intra-observer repeatability of four clinical measurement techniques. Physiotherapy. 1991;77:89-91
- Scham SM, Taylor TKF: Tension signs in lumbar disc prolapse, Clinical Orthopedics 1971;75:195-204
- Toussaint R, Gawlik C, Rehder U, Ruther W. Sacroiliac dysfunction in construction workers. Journal Manipulative Physiological Therapeutics. 1999;22:134-139
- Urban LM: The straight-leg-raising test: a review, Journal of Orthopedics & Sports Physical Therapy 1981;2:117-133
- Viikari-Juntura E, Porras M, Laasonen EM. Validity of clinical tests in the diagnosis of root compression in cervical disc disease. Spine. 1989;14(3):253-257
- Vincent-Smith B, Gibbons P. Inter-examiner & intra-examiner reliability of the standing flexion test. Manual Therapy. 1999;4:87-93
- Vroomen P, deKrom M, Knottnerus J. Consistency of history taking & physical examination in patients with suspected nerve root involvement. Spine. 2000;25:91-97
- Wilkins RH, Brody IA: Lasegue sign, Archives Neurology 1969;21:219-220