


“I think I tore my Rotary Cup!”
Have you ever had a patient say this to you? Although you might get a little chuckle out of the statement, you know what s/he meant. The Rotator Cuff (RC) is made up of four muscles: supraspinatus, infraspinatus, teres minor, and subscapularis. RC tendons can be injured from trauma, over-use, or the aging process. The clustering of signs and symptoms can be valuable in enhancing clinical decision making.
The Predictor Signs of Rotator Cuff Injury: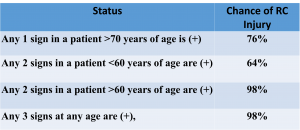
- supraspinatus weakness
- external rotation weakness
- positive impingement test
Both the supraspinatus and infraspinatus are external rotators of the shoulder and have a common attachment to the greater tubercle. Thus, it sense that there are some similar testing procedures.
Supraspinatus Tests
There are several supraspinatus tests in the literature. Clinical practice rarely affords the time to perform more than a couple of tests per structure. In addition, it does not make sense to do tests without ample literature to support them. The tests discussed here for the supraspinatus will include the Full Can, Empty Can, Lateral Jobe, and ER Lag.
 Full Can & Empty Can Tests
Full Can & Empty Can Tests
For the Full Can, the arm is positioned in 30-45° of elevation in the plane of the scapula (scaption). The arm is in external rotation, i.e. the thumb is facing up as if holding a “full can.” The clinician then resists arm elevation in this position.
 The Empty Can, starts in the same position, the plane of the scapula at 30-45° of elevation. However, in the Empty Can test places the arm in internal rotation, i.e. the thumb is rotated downwards as if “emptying a can.”
The Empty Can, starts in the same position, the plane of the scapula at 30-45° of elevation. However, in the Empty Can test places the arm in internal rotation, i.e. the thumb is rotated downwards as if “emptying a can.”
Both the Full Can and Empty Can tests are better as screening tools than as diagnostic tools. This makes sense when the tests incriminates a variety of structures: compressing the subacromial bursa, activating the biceps, stressing the transverse humeral ligament that holds down the biceps, and tractioning the labrum via the attachment to the biceps.
Approximately 24% of supraspinatus tears also involve a tear of the infraspinatus tendon due to the congruent attachment at the anterosuperior edge of the humerus. Full Can and Empty Can tests have been described at various degrees of shoulder elevation. This has led to a wide range of statistical outcomes. In addition, the capability of supraspinatus tests to distinguish between partial- and full-thickness tears is controversial. Somerville et al (2014) identified the critical difference between the results is the choice of the interpretive criterion, i.e. pain versus weakness. Sgroi et al (2018) found weakness correlated better with intraoperative findings. The chart below summarizes these points. So if the Full Can and Empty Can tests are screening tools, are there any supraspinatus tests that are good diagnostic tests? The answer to that question is “yes.”
So if the Full Can and Empty Can tests are screening tools, are there any supraspinatus tests that are good diagnostic tests? The answer to that question is “yes.”
Lateral Jobe
For this test, the patient is in a sitting or standing position and abducts the arm to 90° with IR and 90° of elbow flexion. Thus, the fingers should be pointing inferior and thumb medial. The clinician applies a downward resistance to the distal humerus. This position puts the supraspinatus in a direct line of pull for the proximal and distal attachments. That is in part what makes this a good diagnostic test (sensitivity = 81%, specificity = 89%). But this can be a difficult position to assume for an individual with a supraspinatus injury. One must realize an important fact about all of the orthopedic tests: if you cannot assume the standardized test position, then you can’t render an interpretation of it. In other words, if the standard position is altered, it is inappropriate to say that the test is either positive or negative.
 ER Lag Sign
ER Lag Sign
Another good diagnostic test for the supraspinatus and infraspinatus is the ER Lag Sign. This test places the patient in the plane of the scapula with approximately 90° of elbow flexion. While supporting the elbow, move the patient into a position of just a few degrees shy of full ER. Once there, instruct the patient to hold that position. Release the forearm and note if the patient lags into internal rotation. Failure to maintain the position of ER is a positive test. This test is highly specific (91-100%).
To recap regarding the supraspinatus, although there are several tests in the literature, four have been prioritized: two, the Full Can and the Empty Can, are good screening tools and two, the Lateral Jobe and the ER Lag, are good diagnostic tools.
Infraspinatus Tests
The tests purported to incriminate the infraspinatus, an ER of the shoulder, are the dropping sign, the drop sign, and again the ER Lag. The similarity of some of these test names can make remembering the tests confusing.
Distinguishing supraspinatus and infraspinatus is very challenging. EMG studies have found higher activation of the infraspinatus in actions involving shoulder flexion. In addition, the speed of shoulder movement may be another variable to isolate the infraspinatus. The late cocking phase of baseball pitching has a high infraspinatus to supraspinatus ratio. This raises the possibility that resisted shoulder ER performed via faster isotonic motions may help isolate infraspinatus activity (Hughes, Taylor, & Green, 2015). The infraspinatus may contribute up to 45% of the power of ER.
 Dropping Sign
Dropping Sign
For the dropping sign the patient is seated, the elbow is flexed to 90°, the shoulder at the side (0° of abduction) and 45° of ER. The clinician resists ER. A positive test is dropping into IR. The magnitude of the drop can be recorded to the nearest 5°. A complete tear of the supraspinatus will result in a lag of 5-10°; Complete tears of the supraspinatus and infraspinatus will result in a lag of 15-20°. Clinician should be aware that a drop in the elbow position implicates the supraspinatus; while the arm going into IR implicates the infraspinatus.
Drop Sign
The drop sign is performed in 90° of shoulder abduction with full ER. The patient is asked to hold this position. Inability to maintain the position is a positive test. This has been deemed a good diagnostic test due to the high specificity (100%) and high positive predictive value (100%).
Summary
To recap for the infraspinatus, there are three tests that are all decent diagnostic tools. Although you don’t have to do all three, doing at least two of them would help you to appreciate if the infraspinatus is injured. If one of the two tests selected is the ER Lag, then you probably need to do a third, since the ER Lag also implicates the supraspinatus.
For more cutting edge orthopedic information, explore iOrtho+ Premium Mobile App and please visit https://iortho.xyz/
- Alqunaee M, Galvin R, Fahey T. Diagnostic accuracy of clinical tests for subacromial impingement syndrome: A systematic review & meta-analysis. Archive of Physical Medicine & Rehabilitation. 2012;93:229-236
- Bak K, Sorensen AKB, Jorgensen U, Nygaard M, Krarup AL, Thune C, Sloth C, Pedersen ST. The value of clinical tests in acute full-thickness tears of the supraspinatus tendon: Does subacromial lidocaine injection help in clinical diagnosis? Arthroscopy. 2010;26(6);734-742
- Fowler EM, Horsley IG,Rolf CG. Clinical & arthroscopic findings in recreationally active patients. Sports Medicine, Arthroscopy, Rehabilitation, Therapy, & Technology. 2010;2:2-8
- Gillooly JJ, Chidambaram R, Mok D. The lateral Jobe test: A more reliable method of diagnosing rotator cuff tears. International Journal of Shoulder Surgery. 2010;4(2):41-43
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Hertel R, Ballmer FT, Lambert SM et al: Lag signs in the diagnosis of rotator cuff rupture, Journal of Shoulder Elbow Surgery. 1996;5:307-313
- Hippensteel KJ, Brophy R, Smith MV, Wright RW. A comprehensive review of physical examination tests of the cervical spine, scapula, and rotator cuff. Journal of American Academy of Orthopedic Surgeons. 2018
- Hughes P, Taylor NF, Green R. Identifying shoulder testing positions and movements that isolate infraspinatus from supraspinatus. Journal of Physical Therapy Reviews. 2015;20(2):73-85
- Itoi E, Kido T, Sano A, Urayama M, Sato K. Which is more useful, the full can test or the empty can test in detecting the torn supraspinatus tendon. American Journal of Sports Medicine. 1999;27(1):65-68
- Litaker D, Pioro M, El Bilbeisi H, et al. Returning to the bedside: using history & physical examination to identify rotator cuff tears. Journal of American Geriatric Society. 2000;48:1633-1637
- Lyons AR, Tomlinson JE. Clinical diagnosis of tears of the rotator cuff. Journal of Bone & Joint Surgery. 1992;74-B(3):414-415
- Magee D. Orthopedic Physical Assessment. 5th ed. Philadelphia, PA: WB Saunders Company; 2008.
- McFarland EG, Kim TK. Examination of the shoulder. Thieme Medical Publishers, NY, NY. 2005, pages 152-158
- Miller CA, Forrester GA, Lewis JS. The validity of the lag signs in diagnosing full-thickness tears of the rotator cuff: a preliminary investigation. Archives Physical Medicine Rehabilitation. 2008;89(6):1162-1168
- Minagawa H, Itoi E, Konno N, Kido T, Sano A, Urayama M, Sato K. Humeral attachment of the supraspinatus and infraspinatus tendons: an anatomic study. Arthroscopy. 1998;14(3):302-306
- Neer CS, Welsh RP. The shoulder in sports, Orthopedic Clinics North America. 1977;8:583-591
- Ostor AJ, Richards CA, Prevost AT, Hazleman BL, Speed CA. Interrater reproducibility of clinical tests for rotator cuff lesions. Annals Rheumatic Disease. 2004;63:1288-1292
- Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. Journal of Bone & Joint Surgery. 2005;87-A(7):1446-1455
- Sgroi M, Loitsch T, Reichel H, Kappe T. Diagnostic value of clinical tests for supraspinatus tendon tears. Arthroscopy. 2018;34(8):2326-2333
- Silva L, Andreu JL, Munoz P, et al. Accuracy of physical examination in subacromial impingment syndrome. Rheumatology (Oxford). 2008;47:679-683
- Somerville LE, Willits K, Johnson AM, Litchfield R, LeBel M-E,Moro J, et al. Clinical assessment of physical examination maneuvers for rotator cuff lesions. American Journal of Sports Medicine. 2014;42:1911-1919
- Walch G, Boulahia A, Calderone S et al: The dropping and hornblower signs in evaluating rotator cuff tears, J Bone Joint Surg Br 80:624-628, 1998.