


Cervical Spine Vascular Testing
The vertebral artery is a major artery of the cervical spine. It branches from the subclavian artery, ascends thought the transverse processes of the 6th cervical vertebra foramina, and winds behind the superior articular process of the atlas. The vertebral artery enters the cranium through the foramen magnum where it joins the opposite vertebral artery to form the basilar artery.
The testing procedure(s) of the vertebral artery are reported to reduce the lumen of the vertebral artery, resulting in decreased intracranial blood flow of the contralateral side. This ischemia due to blood loss in the pons and the medulla oblongata can result in dizziness, nausea, syncope, dysarthria, dysphagia, and disturbances of the hearing or vision, paresis or paralysis.
In a meta-analysis published in 2009, Dr. Jeannette Mitchell stated, “Many studies of vertebral artery blood flow changes related to cervical spine rotation have been published, but the findings are controversial and the evidence unconvincing.” Her analysis revealed, blood flow velocity was found to be compromised more in patients than healthy individuals, on contralateral rotation, with the subject sitting. This information is an important to keep in mind as we discuss 5 tests for the vertebral artery.
 The Vertebral Artery Test is performed in supine. The clinician places his/her hands under patient’s occiput to passively move into maximal backward bending, ipsilateral sidebending, and ipsilateral rotation. The position is held for 30 seconds. It is recommended to engage the patient in conversation while monitoring the pupils and affect. A positive test would present with symptoms of vertebrobasilar insufficiency or ischemia (VBI): nausea, dizziness, diplopia, tinnitus, confusion, nystagmus, and/or unilateral pupil changes. The maneuver is repeated to the opposite side.
The Vertebral Artery Test is performed in supine. The clinician places his/her hands under patient’s occiput to passively move into maximal backward bending, ipsilateral sidebending, and ipsilateral rotation. The position is held for 30 seconds. It is recommended to engage the patient in conversation while monitoring the pupils and affect. A positive test would present with symptoms of vertebrobasilar insufficiency or ischemia (VBI): nausea, dizziness, diplopia, tinnitus, confusion, nystagmus, and/or unilateral pupil changes. The maneuver is repeated to the opposite side.
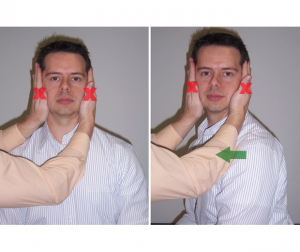 Neck Torsion Test is performed in sitting. A mobile stool is preferred. The clinician sits in front of the patient and holds his/her head as shown (image). While holding the head still, the patient uses the rotating stool to turn his/her body under the stabilized head (image). A positive test would include VBI- related symptoms and incriminate the vertebral artery. However, since the position of the head did not change, a negative test might lead to a suspicion of positional vertigo.
Neck Torsion Test is performed in sitting. A mobile stool is preferred. The clinician sits in front of the patient and holds his/her head as shown (image). While holding the head still, the patient uses the rotating stool to turn his/her body under the stabilized head (image). A positive test would include VBI- related symptoms and incriminate the vertebral artery. However, since the position of the head did not change, a negative test might lead to a suspicion of positional vertigo.
 Hautant Test is performed in a sitting position and is composed of 2 steps. Step #1 is to flex both upper extremities to 90° and hold the position for 10-30 seconds while the eyes are closed. Step #2 is to rotate and extend the neck, then flex both upper extremities to 90° and hold the position for 10-30 seconds while the eyes are closed. The upper extremities are expected to be maintained in the testing position during step #1. Movement during step #1 is not due to a vascular problem. The test is positive when the upper extremities drift during step #2.
Hautant Test is performed in a sitting position and is composed of 2 steps. Step #1 is to flex both upper extremities to 90° and hold the position for 10-30 seconds while the eyes are closed. Step #2 is to rotate and extend the neck, then flex both upper extremities to 90° and hold the position for 10-30 seconds while the eyes are closed. The upper extremities are expected to be maintained in the testing position during step #1. Movement during step #1 is not due to a vascular problem. The test is positive when the upper extremities drift during step #2.
 Barre Test is similar to the Hautant Test but it is performed in standing with both upper extremities flexed to 90°, elbows extended and forearms supinated. The patient is asked to close his/her eyes and hold the position for 10-20 seconds. If 1 arm slowly drifts down and pronates, the test is positive for vascular dysfunction.
Barre Test is similar to the Hautant Test but it is performed in standing with both upper extremities flexed to 90°, elbows extended and forearms supinated. The patient is asked to close his/her eyes and hold the position for 10-20 seconds. If 1 arm slowly drifts down and pronates, the test is positive for vascular dysfunction.
 Finally, the Underburg Test is performed in standing with both upper extremities flexed to 90° with elbows extended and forearms supinated. With this test the eyes are also closed but the cervical spine is extended and rotated right while the patient is asked to march in place for 10 seconds. The test should be repeated with the cervical spine extended and rotated to the left. If in either case 1 arm drops down, the forearm pronates, or there is a loss of balance, the test would be deemed positive for vascular dysfunction.
Finally, the Underburg Test is performed in standing with both upper extremities flexed to 90° with elbows extended and forearms supinated. With this test the eyes are also closed but the cervical spine is extended and rotated right while the patient is asked to march in place for 10 seconds. The test should be repeated with the cervical spine extended and rotated to the left. If in either case 1 arm drops down, the forearm pronates, or there is a loss of balance, the test would be deemed positive for vascular dysfunction.
Of these 5 tests, the only test with statistical data reported is the vertebral artery test. For this test the sensitivity = 0-31%, specificity = 39-86%, (+) likelihood ratio = 0-0.59, and (-) likelihood ratio = 1.16-2.30. Some say that despite not having sensitivity and specificity values, tests that involve a physical response have a slight advantage over those which have a reported response. Further, a positive result does not identify which vertebral artery is the primary culprit. Bulut et al (2016) also demonstrated a loss of cervical lordosis may be associated with vertebral artery hemodynamics. So, in addition to the tests above, one should perform a postural assessment to identify other influential factors.
For more cutting edge orthopedic information, subscribe to iOrtho+ Premium Mobile Web App, at https://iortho.xyz/
- Bulut MD, Alpayci M, Senkoy E, Bora A, Yazmalar L, Yavuz A, Gulsen I. Decreased vertebral artery hemodynamics in patients with loss of cervical lordosis. Medical Science Monitor. 2016;22:495–500.
- Cote PB, Kreitz G, Cassidy JD, Thiel H. The validity of the extension rotation test as a clinical screening procedure before neck
manipulation: a secondary analysis. Journal of Manipulative & Physiological Therapeutics 1996;19(3):159–64. - Evans RC: Illustrated essentials in orthopedic physical assessment, St Louis, 1994, Mosby-Year Books
- Frits-Ritson D. Assessment of cervicogenic vertigo. Journal of Manipulative Physiological Therapeutics. 1991;14:193-198
- Grant R: Vertebral artery testing: the Australian Physiotherapy Association Protocol after 6 years, Manual Therapy. 1996;1:149-153
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Keery R, Tayler AJ. Cervical artery dysfunction assessment & manual therapy. Manual Therapy. 2006;11:243-253
- Kunnasmaa KT, Thiel HW: Vertebral artery syndrome: A review of the literature, Journal Orthopedic Medicine 1994;16:17-20
- Magee D. Orthopedic Physical Assessment. 5th ed. Philadelphia, PA: WB Saunders Company; 2008.
- Maitland GD: Vertebral Manipulation. London, 1973, Butterworths
- Meadows JJ, Magee DJ: An overview of dizziness and vertigo for the orthopedic manual therapist. In Boyling JD, Palastanga N (eds): Grieve modern manual therapy: the vertebral column, 2nd ed. Edinburgh, 1994, Churchill Livingstone.
- Mitchell J. Vertebral Artery Blood flow velocity changes associated with cervical spine rotation: A meta-analysis of the evidence with implications for professional p J Man Manip Ther. 2009;17(1):46-57
- Norre ME. Cervical vertigo: Diagnosis & semiological problem with special emphasis upon cervical nystagmus. Acta Otorhinolaryngol Belgium. 1987;41:436-452
- Ombregt L, Bisschop P, ter Veer HJ, Van de Velde T. A system of orthopedic medicine, London, 1995, W.B. Saunders
- Pettman E: Stress tests of the craniovertebral joints. In Boyling JD, Palastanga N (eds): Grieve Modern Manual Therapy: the vertebral column, 2nd ed. Edinburgh, 1994, Churchill Livingstone.
- Rivett DA, Milburn PD. Effect of premanipulative tests on vertebral artery and internal carotid artery blood flow: a pilot study. Journal of Manipulative & Physiological Therapeutics 1999;22(6):368–76.
- Rivett DA: The premanipulative vertebral artery testing protocol, New Zealand Journal Physiotherapy 1995;23:9-12
- Vidal P, Huijbregts P. Dizziness in orthopedic physical therapy practice: History & physical examination. Journal of Manual & Manipulative Therapy. 2005;12:221-250