

Screening for Hypermobility
We have all heard the term “Double Jointed.” Yet, we know there is no such thing. Joint hypermobility can be the result of repeated activities or trauma. But in this condition, it is usually unilateral. When hypermobility is bilateral, one needs to look for another explanation. How lax is too lax for a joint? The Beighton Scale provides a quantitative criteria for interpretation. The Beighton Scale assesses 9 motions under the premise that systemic hypermobility may imply a connective tissue disorder. The 9 tests are:
-
-
-
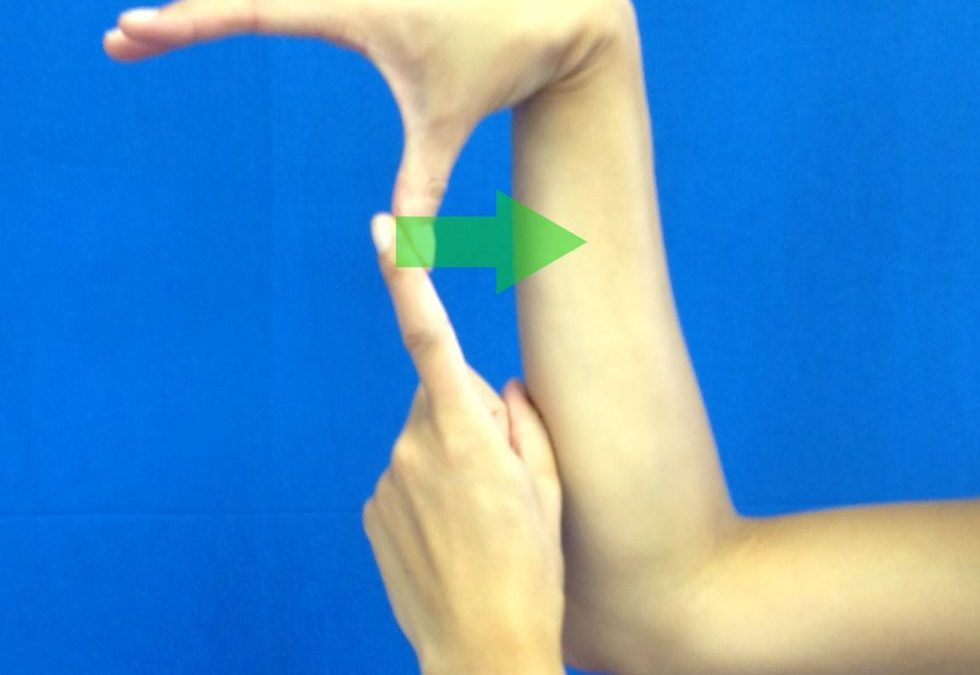
- Right thumb to radius
- Left thumb to radius
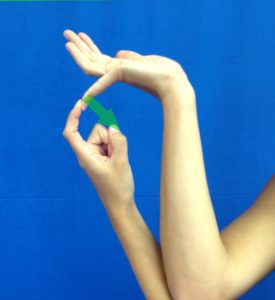
- Right 5th digit hyperextension >90 degrees
- Left 5th digit hyperextension >90 degrees
- Right elbow hyperextension >15 degrees
- Left elbow hyperextension >15 degrees
- Right knee hyperextension >15 degrees
- Left knee hyperextension >15 degrees
- Palms touch the floor with knees straight
-
-
These tests are designed to identify bilateral joint laxity and not erroneously identify systemic laxity in cases where unilateral injuries resulted in hypermobility.




Scoring of the Beighton Test is based on 0 – 9 points. The patient gets one point for each test that is positive. Although there is NO universal agreement on the scoring of the Beighton Scale, the following has been suggested:

 High flexibility may imply congenital ligamentous laxity, i.e. Ehlers-Danlos, Marfans Syndrome. Ehlers-Danlos effects Type I, II, V collagen. These tissues are found in joints, skin, and blood vessels. Beyond the joint laxity, hyperelastic skin and fragile blood vessels are characteristic signs. The vascular fragility can be assessed via a Hess Test. The technique involves inflating a blood pressure cuff to a pressure between systolic and diastolic pressure and maintaining that pressure for five-minutes. If more than 10 petechiae are present with the removal of the blood pressure cuff, the test is considered positive, i.e. capillary fragility.
High flexibility may imply congenital ligamentous laxity, i.e. Ehlers-Danlos, Marfans Syndrome. Ehlers-Danlos effects Type I, II, V collagen. These tissues are found in joints, skin, and blood vessels. Beyond the joint laxity, hyperelastic skin and fragile blood vessels are characteristic signs. The vascular fragility can be assessed via a Hess Test. The technique involves inflating a blood pressure cuff to a pressure between systolic and diastolic pressure and maintaining that pressure for five-minutes. If more than 10 petechiae are present with the removal of the blood pressure cuff, the test is considered positive, i.e. capillary fragility.
Syndromes which as Marfan’s can also present with joint hypermobility. However, other skeletal involvement may include pectus excavatum, an arm span-to-height ratio greater than 1.05, thoracolumbar scoliosis, spondylolisthesis, and a positive thumb sign (thumb and index finger overlap when encircling the opposite wrist). Additional cardiovascular signs may include dilatation of the pulmonary artery and/or dissection of the thoracic or abdominal aorta. Hernia, flat cornea, and myopia may also be present.
The take home message of assessing joint mobility is that unless an individual’s activity involves a symmetrical task consistent with bilateral hypermobility, one should perform a Beighton Test and consider the possibility of a systemic connective tissue disorder. This has a strong impact on the course of intervention. If an individual has a high Beighton score, rehabilitation should focus on joint stabilization, co-contraction, and eccentric control. This would mitigate the individual’s risk of orthopedic injury but one must be cognizant of the many systemic issues that could impact physical performance.
For more cutting edge orthopedic information in iOrtho+ Mobile App, please visit the learning modules at https://iortho.xyz/
- Beighton PH, Solomon L, Soskolne CL. Articular mobility in an African population. Ann Rheum Dis. 1973; 32: 413-417
- Beighton PH Horan F. Orthopedic aspects of the Ehlers-Danlos syndrome. J Bone Joint Surg [Br]. 1969; 51: 444-453.
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Hakim AJ, Grahame R. A simple questionnaire to detect hypermobility: an adjunct to the assessment of patients with diffuse musculoskeletal pain. Int J Clin Pract 2003; 57: 163-166
- Shirley ED, DeMaio M, Bodurtha J. Ehlers-Danlos Syndrome in Orthopedics. SAGE publication, Sept/Oct 2012
- Walsh Flanagan K, Cuppett MM. Medical Conditions in the Athlete, Human Kinetics, 2017