Scaphoid Fracture Detection & Management
Special thanks to DPT students Joo Ho Hong, Zach Jenkins, Taylor Johnson, Lauren Kerner (Widener University Class of 2024)
Identifying and treating a scaphoid fracture is not always a straightforward process. It is common for scaphoid fractures to be missed upon initial radiography, so a negative radiograph is not sufficient in ruling out a scaphoid fracture. Clinical tests to identify a scaphoid fracture include the clamp sign and the axial loading test. The clamp si gn is performed with the wrist pronated and extended while a longitudinal force is applied with ulnar deviation. The axial loading test applies axial compression to the first carpometacarpal (CMC) joint in abduction and extension. Both tests are considered “positive” when pain is reproduced in the anatomic snuffbox (the triangular region on the dorsum of the hand bound by the abductor pollicis longus, extensor pollicis brevis, and the extensor pollicis longus. Of these two tests, the axial loading test has better metrics (sensitivity = 89%; specificity =98%).
gn is performed with the wrist pronated and extended while a longitudinal force is applied with ulnar deviation. The axial loading test applies axial compression to the first carpometacarpal (CMC) joint in abduction and extension. Both tests are considered “positive” when pain is reproduced in the anatomic snuffbox (the triangular region on the dorsum of the hand bound by the abductor pollicis longus, extensor pollicis brevis, and the extensor pollicis longus. Of these two tests, the axial loading test has better metrics (sensitivity = 89%; specificity =98%). 
Depending on the type of fracture, a scaphoid fracture is treated conservatively or with surgery. Non-displaced fractures are typically managed with conservative treatment where one is immobilized in a cast or splint until union of the scaphoid occurs. While one is immobilized, it is appropriate to do range of motion and strengthening exercises proximal and distal to the wrist. This includes active and passive range of motion of the shoulder, elbow, and digits 2-5.
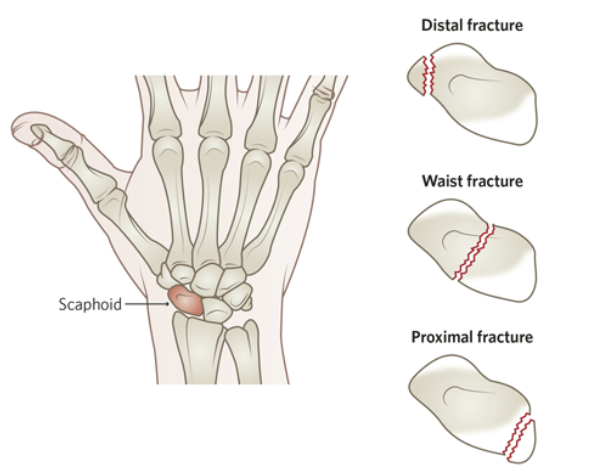
Surgical treatment is usually used for displaced fractures, most commonly in proximal pole scaphoid fractures. The timing of implementing wrist movements is dependent on the amount of time it takes for the union of the scaphoid to occur. If surgery is done to repair the scaphoid one may be in a cast for a shorter period due to increased union rates from surgical fixation. This means they may be able to begin rehabbing the wrist sooner. One should not begin wrist range of motion or thumb range of motion until union occurs because this can lead to improper healing resulting in poor outcomes.
Once the scaphoid union occurs and the cast or splint is removed one can begin range of motion movements at the wrist and thumb. Gentle active assisted, active and passive range of motion exercises can be done for wrist and thumb flexion and extension, along with radial and ulnar deviation of the wrist and thumb opposition, abduction, and adduction. One can also do gentle stretching of wrist flexors and extensors to help stretch the muscles that have been impacted by immobilization. Wrist flexion and extension motions can be done without resistance initially and then progressed to use dumbbells or resistance bands as tolerated. Pronation and supination exercises can also be done and progressed with dumbbells. Grip strength movements should also be incorporated as tolerated through ball squeezes or with putty. Progressive resistance exercises should be guided by pain tolerance.
Throughout the healing process modalities such as ice and heat can be used to help relieve symptoms such as stiffness, swelling, or pain associated with the fracture. Joint and soft tissue mobilization can also be valuable in restoring optimal function.
For more cutting-edge orthopedic information on iOrtho+ PREMIUM Web App, please visit the learning modules at https://iortho.xyz/
If you would like to learn more about the Mobil–Aider Arthrometer to quantify joint mobility, please visit: https://iortho.xyz/
References:
-
Arsalan-Werner A, Sauerbier M, Mehling IM. Current concepts for the treatment of acute scaphoid fractures. European Journal of Trauma and Emergency Surgery. 2015;42(1):3-10.
-
Karpouzos A, Diamantis E, Farmaki P, et al. Nutritional Aspects of Bone Health and Fracture Healing. J Osteoporosis. 2017; 2017: 4218472. doi: 10.1155/2017/4218472
-
Lane R, Tafti D, Varacallo M. Scapholunate Advanced Collapse. [Updated 2022 Feb 12].In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 May Availablefrom: https://www.ncbi.nlm.nih.gov/books/NBK537124/2022. Scaphoid Fracture. [online] Available at: <https://www.physiopedia.com/Scaphoid_Fracture> [Accessed 29 May 2022].
-
Powell JM, Lloyd GJ, Rintoul RF. New clinical test for scaphoid fracture of the scaphoid. Canadian Journal of Surgery. 1988;31:237-238
-
Waeckerle JF. A prospective study identifying the sensitivity of radiographic findings & the efficiency of clinical findings in carpal navicular fractures. Annals Emergency Medicine. 1987;16:733-737
-
Werner FW, St-Amand H, Moritomo H, Sutton LG, Short WH. The Effect of Scaphoid Fracture Site on Scaphoid Instability Patterns. Journal of Wrist Surgery. 2016;5(1):47-51.