


Provocation Tests
On occur, we are faced with individuals who present with a signs or symptoms that are inconsistent. It may be hard to determine if they are experiencing severe pain, non-organic signs, or are if there is magnification of the condition. The Waddell’s sign, Hoover test, and Sign of the Buttocks may be able to help you.
Waddell’s sign was first described by Professor Gordon Waddell to identify patients who underwent low back surgery and were likely to have a poor prognosis. Somewhere in the use and/or publication of these signs, there was misinterpretation. Clinicians began to use the signs as a clinical or legal test to detect malingering.
Waddell’s sign consists of 8 clinical physical signs that are labeled “non-organic signs.” Waddell was not implying pain was not real. His intent was to bring to light the psychosocial context of back pain to guide clinicians to incorporate psychosocial and behavior management into the physical treatment of back pain. The chart below identified the physical signs, the testing technique, and the criteria for a positive test.
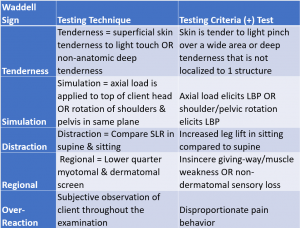
Three or more of the 5 Waddell components must be present for the test to be considered positive. Waddell’s Sign reports interrater reliability of 80%, intrarater reliability of 85%, reliability (ICC) of 0.74, and SEM = 1.7. Waddell also has a Disability Index: http://oml.eular.org/sysModules/obxOML/docs/id_58/addel%20Disability%20Index_english.pdf
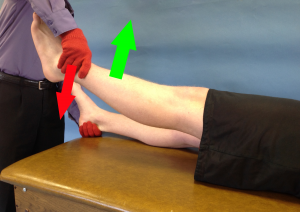 Hoover Test is used to assess for functional weakness of hip extensors or malingering. This test is performed in a supine position. The clinician places a hand under the heel of contralateral leg and resists a SLR on the ipsilateral leg.
Hoover Test is used to assess for functional weakness of hip extensors or malingering. This test is performed in a supine position. The clinician places a hand under the heel of contralateral leg and resists a SLR on the ipsilateral leg.
A (+) test is a lack of downward (extension) pressure on the contralateral leg. This is suggestive that there is functional weakness or the attempt to raise the leg was not genuine. The metric for the assessment of functional weakness are sensitivity = 63% and specificity = 100%. There are no metrics associated with a non-genuine effort.

 Sign of the Buttock was a concept developed by Cyriax. It is no 1 test. It is 7 signs that when combined indicate serious pathology. When positive, it is considered a “reg flag.”
Sign of the Buttock was a concept developed by Cyriax. It is no 1 test. It is 7 signs that when combined indicate serious pathology. When positive, it is considered a “reg flag.”
The 7 signs include:
- Buttock is swollen and tender to palpation
- Straight Leg Raise is limited and painful
- Trunk flexion is limited
- Hip flexion with knee flexion limited and painful
- Hip flexion has an empty end feel
- Hip has a non capsular pattern of restriction (flex,abd,IR)
- Resisted hip movements are painful and weak (especially hip extension)
To perform the Sign of the Buttock, the patient is in a supine position. The clinician then passively performs a SLR and notes the greatest degree of hip flexion before limitation or onset of symptoms occurs. The knee is then flexed and further hip flexion is attempted. The degree of available hip flexion is compared with and without the knee flexed.
A (+) test is when hip flexion with knee flexion is not greater than a SLR (hip flexion without knee flexion). The interpretation is there is a non-musculoskeletal cause for the patient’s symptoms. Unfortunately there is no statistical data on this test.
![]() For more clinical tests that include images and videos, please subscribe to iOrtho+ Premium Web App. More cutting edge orthopedic information can be found at https://iortho.xyz/
For more clinical tests that include images and videos, please subscribe to iOrtho+ Premium Web App. More cutting edge orthopedic information can be found at https://iortho.xyz/
- Burns SA, Burshteyn M, Mintken PE. Sign of the Buttock Following Total Hip Arthroplasty. Journal Orthopedic & Sports Physical Therapy 2010;40(6):377
- Cook C. Physical Examination Tests for Neurological Screening. In: Cook C, Hegedus E. Physical Examination Tests: An Evidence Based Approach. Upper Saddle River, NJ; Prentice Hall: 2008
- Cyriax, J. Textbook of Orthopedic Medicine
- Davidson M, Keating JL: A comparison of five low back disability questionnaires: reliability and responsiveness, Physical Therapy. 2002;82(1):8-24
- Greenwood MJ, Erhard RE, Jones DL. Differential diagnosis of the hip vs. lumbar spine: five case reports. Journal Orthopedic & Sports Physical Therapy. 1998;27(4):308-315
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Koehler PJ, Okun MS. Important observations prior to the description of the Hoover sign. Neurology 2004 Nov; 63 (9): 1693-1697.
- Main CJ, Waddell G. Behavioral responses to examination. A reappraisal of the interpretation of nonorganic signs. Spine. 1998;23(21):2367-2371
- McWhirter L, Stone J, Sandercock P, Whiteley W. Hoover’s sign for the diagnosis of functional weakness: a prospective unblinded cohort study in patients with suspected stroke. J Psychosom Res. 2011 Dec;71(6):384-386.
- Stone, Jon, Sharpe, Michael. Hoover’s Sign. Practical Neurology. 2001 Nov; 50.
- Ziv I, Djaldetti R, Zoldan Y, Avraham M, Melamed E. Diagnosis of non-organic limb paresis by a novel objective motor assessment: the quantitative Hoover test. J. Neurol. 1998 Dec;245 (12): 797-802.