
![]()

Impingement Tests of the Hip
Femoro-Acetabular Impingement
Hip impingement, also known as femoro-acetabular impingement (FAI), was first described by Smith-Petersen (1936). FAI is a condition in which there is abnormal and wearing contact between the ball and socket of the hip joint. The result is increased friction during hip movements that damage the joint. Individuals who are at risk tend to be younger individuals active in tasks involving pivoting with internal rotation. For example, gymnastics, soccer, hockey, and swimming breaststroke are activities that fulfill the risk criteria.
There are two types of FAI: cam and pincer. Cam impingement is an osseous abnormality (bone bump) at the femoral head-neck junction. It is an abnormality of the femur and the impact can damage the articular cartilage. Pincer impingement is an abnormality of the bony acetabulum leading to over-coverage of the femoral head, i.e. acting like tweezers or pincers around the femoral head. This damages the labrum. There are two animated videos on “youtube” that describe the differences in these types of FAI:
- CAM = http://www.youtube.com/watch?v=qkVxHnCyuxc
- PINCER = http://www.youtube.com/watch?v=qu5DAJCZjyA
FAI Signs & Symptoms 

Patients often complain of pain in the groin after prolonged sitting or walking. Many athletes describe pain in the groin with deep flexion or rotation of the hip during activity. Occasionally, a popping or clicking in the front of the hip is described. Pain may also radiate along the lateral thigh and in the buttocks. The C-sign was described by Byrd (2005) and is a simplistic indication of FAI. The patient makes a shape of a ‘C’ with his/her hand and places the hand right on the hip joint, i.e. the location of the pain. It is important to rule out other causes of pain in this area which may originate in the low back or abdomen.
FAI Clinical Tests
Many of the physical tests for FAI are very similar. As one might expect, they incorporate common motions or positions. These tests are: the DEXRI, DIRI, impingement, FAbER, and FAdIR.
 DEXRI & DIRI Tests
DEXRI & DIRI Tests 
The DEXRI (Dynamic External Rotation Impingement) and DIRI (Dynamic Internal Rotation Impingement) tests involve scouring the hip through a defined arc of motion. The DEXRI is performed in supine with the involved leg flexed to 90° at the hip and knee. The hip is passively taken through an arc of hip abduction and ER. The DIRI is also performed in supine with the involved leg flexed to 90° at the hip and knee but the hip is passively taken through an arc of hip adduction and IR. Some clinicians recommend holding the contralateral limb in a flexed position beyond 90 degrees to stabilize the pelvis. Together, these two tests function to scour the entire hip socket. Unfortunately, neither test has any statistical data reported to identify it as a screening or diagnostic tool.
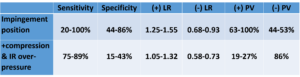
Impingement Test 
Likewise, the impingement test attempts to reproduce pain into the groin. In supine, the patient is passively taken into a position of hip/knee flexion to 90/90 and then into IR (no adduction). Some clinicians recommend adding axial compression and/or over-pressure into IR. However, these additional maneuvers do not appear to enhance the statistical values.
 FAbER & FAdIR Tests
FAbER & FAdIR Tests
The FAbER (Flexion, Abduction, External Rotation) and FAdIR (Flexion, Adduction, Internal Rotation) tests are similar to the DEXRI and DIRI tests with regard to the combination of motions. The FAbER test, also known as the Patrick test, is used to assess a wide array of musculoskeletal problems: hip/SI pathology, labral damage, or FAI. The position is known as the “figure – 4” position. In supine, the patient is passively taken into a position of hip flexion, abduction, and ER hip, i.e involved ankle is placed on opposite knee. The lateral malleolus is placed on the contralateral distal thigh. Overpressure is applied to the medial border of the flexed knee. Given the number of tissues challenged by the FAbER test, a positive test can take many forms. Pain assuming the position may be due to a problem with the Sartorius muscle. Pain once in the position may be due to hip impingement or SI/low back pathology. If the knee is more than 4 cm from the surface, the labrum may be the problem. Thus, regardless of the tissue being tested, the FAbER test, by itself, is a poor diagnostic tool.
The FAdIR is performed in supine just like the DIRI. The hip and knee is passively flexed to 90/90 and the adducted with hip IR. As the femoral head comes in contact with the acetabular rim, a positive test for FAI would be pain in the groin region. The FAdIR test only has statistics for sensitivity and the value is high (88-100%). Likewise, when the FAbER and FAdIR are both negative, sensitivity is 90-100% (excellent screening combination).
Summary
Although none of these tests are strong diagnostic tools, they can be used to rule-out impingement. If these tests are positive, the mechanism of injury and the pain referral pattern may help to confirm the diagnosis.
For more cutting edge orthopedic information in iOrtho+ Premium Mobile App, please visit https://iortho.xyz/
Subscribe for the low annual rate of only $9.99. If you prefer to try iOrtho+ Premium Mobile App for 1 month, you can do so for only $1.99.
FYI – Prior blog posts are available at https://iortho.xyz/
- Ayeni O, Chu R, Hetaimish B, Nur L, Simunovic N, Farrokhyar F, Bedi A, Bhandari M. A painful squat test provides limited diagnostic utility in CAM-type femoroacetabular impingement. Knee Surgery, Sports, Trauma, Arthroscopy. 2014;22:806-811
- Beaule P, Zaragoza E, Motamedi K, Copelan N, Dorey FJ. Three-dimensional computed tomography of the hip in the assessment of femoracetabular impingement. Journal of Orthopedic Research. 2005;23:1286-1292
- Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement Part II. Clinical Orthopedics. 2004;41:67-73
- Burnett RSJ, Della Rocca GJ, Prather H, Curry M, Maloney WJ, Clohisy JC. Clinical presentation of patients with tears of the acetabular labrum. Journal of Bone and Joint Surgery. 2006;88A:1448-1457
- Byrd JWT, Jones KS. Traumatic rupture of the ligamentum teres as a source of hip pain. Arthroscopy: Journal of Arthroscopic & Related Surgery. 2004;20(4):385-391
- Clohisy JC, Knaus ER, Hunt DM, Lesher JM, Harris-Hayes M, Prather H. Clinical Presentation of Patients with Symptomatic Anterior Hip Impingement. Clinical Orthopaedics & Related Research. 2009;467(3):638-644
- Gulick DT. iOrtho+ Premium Web App. DTG Enterprises LLC. 2025
- Gulick, DT. OrthoNotes, 5th FA Davis Publishing, Philadelphia. 2023
- Hananouchi T, Yasui Y, Yamamoto K, Toritsuka Y, Ohzono K. Anterior impingement test for the labral lesions has high positive predictive value. Clinical Orthopedic & Related Research. 2012;470:3524-3529.
- Hase T, Ueo T. Acetabular labral tear: Arthroscopic diagnosis and treatment. 1999;15:138-141
- Ito K, Leunig M, Ganz R. Histopathologic features of the acetabular labrum in femoroacetabular impipngement. Clinical Orthopedic. 2004;429:262-271
- Kassarjian A, Yoon LS, Belzile E, Connolly SA, Millis MB, Palmer WE. Triad of MR arthrographic findings in patients with cam-type femoracetabular impingement. 2005;236:588-592
- Kuhlman GS, Domb BG. Hip impingement: Identifying and treating a common cause of hip pain. American Family Physician. 2009 Dec;80(12):1429-1434
- Leibold MR, Huijbregts PA, Jensen R. Concurrent Criterion-Related Validity of Physical Examination Tests for Hip Labral Lesions: A Systematic Review. Journal of Manual & Manipulative Therapy. 2008;16(2):E24-41
- Leuig M, Podeszwa D, Beck M, Werlen S, Ganz R. Magnetic resonance arthrography of labral disorders in hips with dysplasia and impingement. Clinical Orthopedics. 2004;418:74-80
- Magee D. Orthopedic Physical Assessment. 5th ed. Philadelphia, PA: WB Saunders Company; 2008.
- Martin RL, Sekiya JK. The interrater reliability of 4 clinical tests used to assess individuals with musculoskeletal hip pain. Journal Orthopedics Sports Physical Therapy. 2008 Feb;38(2):71-77
- Maslowski E, Sullivan W, Forster Harwood J, Gonzalez P, Kaufman M, Vidal A, Akuthota V. The diagnostic validity of hip provocation maneuvers to detect intra-articular hip pathology. Physical Medicine & Rehabilitation. 2010 Mar; 2(3): 174-181
- Narvani AA, Tsiridis E, Kendall S, Chaudhuri R, Thomas P. A preliminary report on prevalence of acetabular labral tears in sports patients with groin pain. Knee Surgery, Sports & Traumatological Arthroscopy. 2003;11:403-408
- Nogier A, Bonin N, May O, et al. Descriptive epidemiology of mechanical hip pathology in adults under 50 years of age. Prospective series of 292 cases: Clinical & radiological aspects & physiopathological review. Orthopedic Traumatology & Surgical Research. 2010;96:S253-S258
- Pacheco-Carrillo A, Medina-Porqueres I. Physical examination tests for the diagnosis of femoroacetabular impingement: A systematic review. Physical Therapy in Sport. 2016
- Philippon MJ, Briggs KK, Yen YM, Kuppersmmith DA. Outcomes following hip arthroplasty for femoroacetabular impingement with associated chondrolabral dysfunction: Minumum two-year follow-up. Journal of Bone & Joint Surgery (British). 2009;91:16-23
- Plante M, Wallace R, Busconi BD. Clinical diagnosis of hip pain. Clinical Sports Medicine. 2011;30(2):225-238
- Santori N, Villar RN. Acetabular labral tears: Result of arthroscopic partial limbectomy. Arthroscopy. 2000;16:11-15
- Sink EL, Gralla J, Ryba A, Dayton M. Clinical presentation of femoroacetabular impingement in adolescents. Journal of Pediatric Orthopedics. 2008;28:806-811
- Tijssen M, van Cingel R, Willemsen L, de Visser E. Diagnosis of femoroacetabular impingement & labral pathology of the hip: a systematic review of the accuracy & validity of physical tests. 2012;28(6):860-861
- Tranovich MJ, Salzler MJ, Enseki KR, Wright VJ. A review of femoroacetabular impingement & hip arthroscopy in the athlete. Physician & Sportsmedicine. 2014 Feb;42(1):75-87