
![]()

Acromio-Clavicular Injuries
The most common mechanism of injury to the acromioclavicular (AC) and coracoclavicular (CC) ligaments is a direct force applied to the superior aspect of the acromion, usually from a fall with the upper extremity in an adducted position. Falling on an outstretched hand or elbow may also lead to AC joint separation. AC joint injuries account for more than forty percent of all shoulder injuries. Physical examination may reveal edema, bruising, and/or a deformity of the AC joint depending on the degree of injury. There are three classifications of injury based on the magnitude of the damage:
- Type I = AC ligament is slightly torn, but there’s no damage to the CC ligament is unharmed.
- Type II = AC ligament is completely torn, and there’s little or no tear to the CC ligament.
- Type III = both AC and CC ligaments are completely torn.
The clinical tests used to assess the AC joint serve as an excellent example of the value of clustering test results. These tests include the AC shear, Paxinos, Cross-body adduction, & AC resistance test.
AC Shear Test 
The AC shear is a simple test that has been around for quite some time: the literature dates back to the early 1980s on this test. The technique entails “smushing” the AC joint together to create a shearing force. By interlacing his/her fingers, the clinician places the heel of one hand on the front of the AC joint and the heel of the other hand on the back of the AC joint. Now the AC joint is surrounded and the clinician squeezes his/her hands together. A positive test is pain or excessive movement at the AC joint. Given the small amount of motion, to confirm the concept of “excessive movement,” a bilateral comparison should be performed.
Paxinos Sign 
The Paxinos sign is a more current version of the AC shear test. For this test, one palpates the posterior acromion and the lateral aspect of the clavicle. If the clinician places his/her thumb of one hand over the posterior acromion and index or long finger of the other hand over the lateral aspect of the clavicle, a compression force will shear the AC joint. At first look, the Paxinos appears to be more precise with specific palpation of the structures involved as opposed to a gross motor task of the AC shear test. However, it has been this author’s impression the reason the metrics for the Paxinos may not be as strong as that of the AC shear could be the inability to generate sufficient force with the fingers to create enough shear to be diagnostic.
 Cross-body Adduction Test
Cross-body Adduction Test
The Cross-body Adduction test involves horizontal adduction of the arm in a position of interior rotations (IR). A positive test is pain at the AC joint. However, this maneuver may also incriminate the labrum, bursa, and/or rotator cuff. Thus, confirming the exact location of the discomfort with the patient is important.
AC Resisted Test 
This test is performed in a seated position with the shoulder flexed to 90°, maximal IR, and 90° of elbow flexion, the client is asked to horizontally abduct the arm against resistance (Figure 4). Again, a positive test is pain at the AC joint.
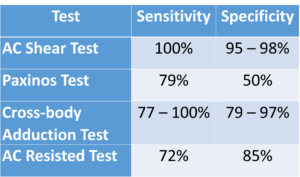
AC Test Statistics
Metrics for the four AC joint tests are as follows:
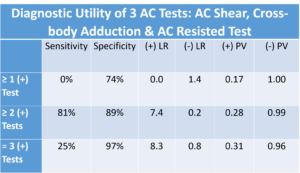
In 2004, a study by Chronopoulus, Kim, Park et al looked at putting these tests for the AC joint into clusters. The chart below summarizes their work. As you can see, if one of the three tests studied (AC shear, cross-body adduction, & AC resisted test) were positive, you have a 74% chance of accurately diagnosing an AC injury. If two or more of the tests are positive, you can see that the specificity increases to 89% and (+) likelihood ratio increased to 7.4. Furthermore, if three or more of the tests are positive, specificity increases again to 97% and the (+) likelihood ratio to 8.3. This makes the clustering of these tests very strong diagnostic predictors for AC joint pathology.
In summary, the clinical decisions made on the implementation of orthopedic tests need to be based on statistical data if it is to be “evidence-based.” AC tests provide excellent data for confident decision-making. For more cutting edge orthopedic information or iOrtho+ Premium Mobile App, please visit https://iortho.xyz/
For more cutting edge orthopedic information in iOrtho+ Premium Mobile App, please visit https://iortho.xyz/
Subscribe for the low annual rate of only $9.99. If you prefer to try iOrtho+ Premium Mobile App for 1 month, you can do so for only $1.99.
FYI – Prior blog posts are available at https://iortho.xyz/
Information on the Mobil-Aider Arthrometer to quantify joint mobility can be found at https://iortho.xyz/
- Axe MJ. Acromioclavicular joint injuries in the athlete, Sports Medicine Arthroscopy Reviews. 2000;8:182-191
- Calis M, Akgun K, Birtane M, Karacan I, Calis H, Tuzun F. Diagnostic values of clinical diagnostic tests in subacromial impingement syndrome. Annuals of Rheumatic Disease. 2000;59(1):44-47
- Chronopoulus E, Kim TK, Park HB et al. Diagnostic value of physical tests for isolated chronic acromioclavicular lesions, HB American Journal Sports Medicine. 2004;32(3):655-661
- Clark HD, McCann PD. Acromioclavicular joint injuries, Orthopedic Clinics North America. 2000;31:177-187
- Davies GJ, Gould JA, Larson RL. Functional examination of the shoulder girdle, Physical Therapy Sports Medicine. 1981;9:82-104
- Dutton M. Orthopedic examination, evaluation & intervention, New York, McGraw Hill, 2004
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC, 2025
- Gulick, DT. OrthoNotes, 5th FA Davis Publishing, Philadelphia, 2023
- Murell GAC. How to treat shoulder dysfunction. Australian Doctor. 2004;17:23-30
- Obrien SJ, Pagnani M, Fealy S, McGlynn S, Wilson J. The active compression test: A new & effective test for diagnosing labral tears & acromioclavicular joint abnormality. American Journal of Sports Medicine. 1998;26:610-614
- Ostor AJ, Richards CA, Prevost AT, Hazleman BL, Speed CA. Interrater reproducibility of clinical tests for rotator cuff lesions. Annals Rheumatic Disease. 2004;63:1288-1292
- Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. Journal of Bone & Joint Surgery. 2005;87-A(7):1446-1455
- Powell JW, Huijbregts PA. Concurrent Criterion-Related Validity of Acromioclavicular Joint Physical Examination Tests: A Systematic Review. The Journal of Manual & Manipulative Therapy. 2006;14(2):E19 – E29
- Shaffer BS: Painful conditions of the acromioclavicular joint, Journal American Academy Orthopedic Surgery 1999;7:176-188
- Walton J, Mahajan S, Paxinos A, et al. Diagnostic value of tests for acromioclavicular joint pain. Journal of Bone & Joint Surgery. 2004;86-A:807-812