
 Top 5 Biomechanical Faults that Lead to Knee Injuries…..And How to Fix Them
Top 5 Biomechanical Faults that Lead to Knee Injuries…..And How to Fix Them
Knee injuries are rarely just a “knee” problem. Faulty biomechanics are often driven by weakness, poor neuromuscular control, or limited mobility in adjacent joints and commonly contribute to knee pain and dysfunction. Here are five of the most common culprits and how to address them:
1. Dynamic Knee Valgus is the inward collapse of the knee during weight-bearing activities like squats, jumping, or running. This can easily be observed in the “dynamic valgus jump test.”
Common causes:
-
Weak gluteus medius and maximus
-
Poor ankle dorsiflexion
-
Excessive femoral internal rotation
-
Hip adductor dominance
How to fix it:
-
Strengthen hip abductors (e.g., side-lying clamshells, lateral band walks)
-
Improve ankle mobility (e.g., ankle dorsiflexion mobilizations)
-
Cue proper knee alignment during functional tasks (e.g., “knee over second toe”)
2. Quad Dominance with Poor Hip Strategy is the over-reliance on the quadriceps, especially during landings, stairs, and squats, with limited hip engagement.
Common causes:
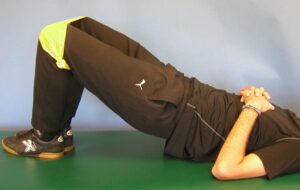
OLYMPUS DIGITAL CAMERA
-
Weak posterior chain (glutes, hamstrings)
-
Poor hip hinge mechanics
-
Fear of forward trunk lean in athletes
How to fix it:
-
Teach and train the hip hinge pattern (e.g., RDLs, kettlebell swings)
-
Glute bridges, hip thrusts, and single-leg RDLs
-
Promote forward trunk lean in safe, controlled settings (e.g., box jumps, lunges)
3. Poor Tibial Control (excessive internal rotation or lateral shift) is a misalignment or twisting of the tibia relative to the femur during dynamic activity.
Common causes: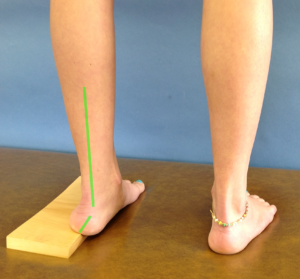
-
Poor control of foot pronation can be identified with the Coleman Block Test
-
Imbalances between medial and lateral quad/hamstring activation
-
Weak hip and ankle coordination
How to fix it:
-
Strengthen foot intrinsic and posterior tibialis
-
Address proximal and distal sequencing via closed-chain coordination drills
-
Consider foot orthotics or taping in high-risk individuals
4. Limited Ankle Dorsiflexion can cause compensatory knee and hip mechanics, especially during squatting or landing.
Common causes:
-
Tight soleus/gastrocnemius
-
Posterior ankle capsule restriction
-
Previous ankle sprains
How to fix it:
-
Mobilizations (banded joint mobilizations, manual therapy)
-
Soft tissue work and foam rolling
-
Functional dorsiflexion drills (e.g., knee-to-wall test exercises)
5. Asymmetrical or Delayed Neuromuscular Activation can include uncoordinated or delayed firing of stabilizers and prime movers during movement.
Common causes:
-
Post-injury compensations (e.g., post-ACL surgery)
-
Motor control deficits
-
Poor proprioceptive input
How to fix it:
-
Re-train single-leg balance and stability (e.g., Y-balance, Bosu drills)
-
Include perturbation training and reactive stability tasks
-
Biofeedback training to enhance timing and symmetry