 Quantifying Pectoralis Muscle Tightness
Quantifying Pectoralis Muscle Tightness 
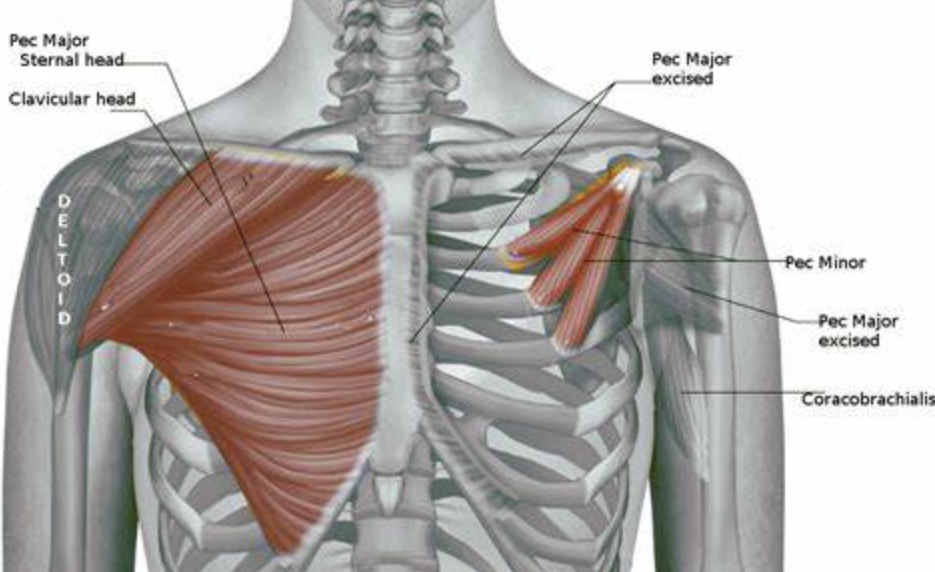
The pectoralis is the fan-shaped muscle that covers the upper part of the chest. The pectoralis major has a clavicular and a sternocostal head. The clavicular head arises from the anterior, medial half of the clavicle, while the sternocostal head comes off the anterior sternum and the ribs 1 to 6. Both heads of the pectoralis major attach to the bicipital groove of the humerus.
The pectoralis major muscle performs 3 actions:
Because of the way we function with most activities of daily living occurring in front of us, the pectoralis muscles tend to get tight. Significant imbalance can occur between our anterior and posterior musculature. Anterior (Rounded) shoulder displacement influences our posture, our breathing, and can limit shoulder mobility. The orientation of the 2 heads of the pectoralis major muscle require separate assessment techniques to ascertain tightness.

 For the clavicular portion, the patient lies in supine with the finger interlaced behind the head. The elbows are allowed to drop down to the table as much as possible. Using a tape measure, the distance from olecranon process of the elbow to the table is recorded bilaterally.
For the clavicular portion, the patient lies in supine with the finger interlaced behind the head. The elbows are allowed to drop down to the table as much as possible. Using a tape measure, the distance from olecranon process of the elbow to the table is recorded bilaterally.

 For the sternal portion, the patient lies in supine with the upper extremities passively abducted to 135° with shoulder external rotation. The elbows are extended and forearms supinated. A tape measure is used to measure the distance from the lateral epicondyle to the table.
For the sternal portion, the patient lies in supine with the upper extremities passively abducted to 135° with shoulder external rotation. The elbows are extended and forearms supinated. A tape measure is used to measure the distance from the lateral epicondyle to the table.
When comparing bilaterally, asymmetry may need to be addressed. The intrarater reliability for these techniques is 81 – 84%.
The pectoralis minor originates from the coracoid process of the scapula and attaches to the anterior aspect of ribs 3, 4, and 5. The function of the pectoralis minor includes: 
 The pectoralis minor can become very tense when the serratus anterior is weak. Likewise, shortening of pectoralis minor may produce impingement on blood vessels and nerves, causing shoulder impingement and thoracic outlet syndrome. To assess for pectoralis minor tightness, the patient is placed in a supine position with both arms are the side. The arms should be in anatomic position, i.e. shoulders externally rotated, elbows extended, and forearms supinated. A tape measure is used to measure the distance from the posterior border of the acromion to the table. This measure should be taken bilaterally. Asymmetry is considered a positive test. The intrarater reliability for these techniques is 81 – 83%.
The pectoralis minor can become very tense when the serratus anterior is weak. Likewise, shortening of pectoralis minor may produce impingement on blood vessels and nerves, causing shoulder impingement and thoracic outlet syndrome. To assess for pectoralis minor tightness, the patient is placed in a supine position with both arms are the side. The arms should be in anatomic position, i.e. shoulders externally rotated, elbows extended, and forearms supinated. A tape measure is used to measure the distance from the posterior border of the acromion to the table. This measure should be taken bilaterally. Asymmetry is considered a positive test. The intrarater reliability for these techniques is 81 – 83%.
Assessment of the pectoralis major and minor is important to identify the underlying problem related to shoulder or postural dysfunction and help restore muscle balance.
More cutting-edge orthopedic information can be found in iOrtho+ Premium Mobile App. Subscribe for the low annual rate of only $9.99. If you prefer to just try iOrtho+ Premium for 1 month, you can do so for only $1.99 Please visit https://iortho.xyz/Prior blog posts are also available at https://iortho.xyz/
- Borstad JD. Resting position variables at the shoulder: Evidence to support a posture-improvement association. Physical Therapy. 2006;86:549-557
- Gulick DT. iOrtho+ Premium Web App. DTG Enterprises LLC. 2024
- Gulick, DT. OrthoNotes, 5th FA Davis Publishing, Philadelphia. 2023
- Manske RC, Jones SM, Bryan TL, et al. Intrarater & interrater reliability of upper extremity muscle length testing & a comparison of upper extremity muscle length in normal males & college baseball pitchers. JOSPT. 2006;36(1):A83
- Reiman MP, Manske RC. Functional Testing in Human Performance. Champaign, IL: Human Kinetics, 2009
Reese NB, Bandy WD. Joint Range of Motion & Muscle Length Testing. Philadelphia: Saunders, 2002