
![]() Deep Tendon Reflexes by the Numbers
Deep Tendon Reflexes by the Numbers 
Deep Tendon Reflexes (DTR) are graded by numbers. They represent a numerical segment of the spine and their clinical value is indicated by numbers such as sensitivity, specificity, and likelihood ratios. So we are dealing with numbers all around!
DTRs are a brisk muscle contraction in response to a sudden stretch generated by a reflex hammer tapping the tendon insertion. DTRs assess the central nervous system as well as the peripheral nervous system at the segmental level of innervation. Hyperactive reflexes may indicate pathology above the level of the reflex arc. Hypoactive reflexes may be the result of muscle, nerve, nerve root, or spinal cord damage.
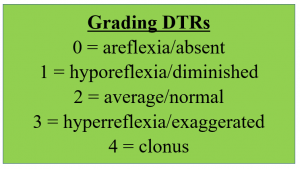 DTRs only take a few seconds to perform and require minimal equipment. The grading of the DTRs is from 0 to 4 as displayed.
DTRs only take a few seconds to perform and require minimal equipment. The grading of the DTRs is from 0 to 4 as displayed.
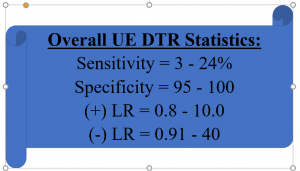 The overall upper extremity reflexes can be good diagnostic tools for the detection of neurological lesions. In addition, data published by Teitelbaum et al (2002) stated that when DTRs are used for the detection of unilateral cerebral lesions the statistics are as follows: Sensitivity = 68.9%; Specificity = 87.5%; (+) LR = 5.5; (-) LR = 0.36; (+) PV = 86.1%; (-) PV = 71.4%.
The overall upper extremity reflexes can be good diagnostic tools for the detection of neurological lesions. In addition, data published by Teitelbaum et al (2002) stated that when DTRs are used for the detection of unilateral cerebral lesions the statistics are as follows: Sensitivity = 68.9%; Specificity = 87.5%; (+) LR = 5.5; (-) LR = 0.36; (+) PV = 86.1%; (-) PV = 71.4%.
Let’s look at the performance of each of the DTRs for the upper and lower extremities. Upper extremity reflexes include the biceps, brachioradialis, and triceps to assess C5-6, C5-6, and C6-8, respectively. Whereas, the lower extremity reflexes are the patella, tibialis posterior, medial hamstrings, lateral hamstrings, and Achilles to assess L2-4, L4–5, L5–S1, S1–2, and S1–2, respectively. The performance of these reflexes are as follows:
 Biceps: Position the patient with the arm supported. By cradling the elbow and draping the patient’s forearm over your arm, the biceps muscle can be relaxed. The clinician identifies the bicep tendon in the crease of the elbow and taps the biceps tendon with a reflex hammer.
Biceps: Position the patient with the arm supported. By cradling the elbow and draping the patient’s forearm over your arm, the biceps muscle can be relaxed. The clinician identifies the bicep tendon in the crease of the elbow and taps the biceps tendon with a reflex hammer.
 Brachioradialis: Position the patient with the arm supported. By cradling the elbow and draping the patient’s forearm over your arm, the brachioradialis muscle can be relaxed. The clinician taps the brachioradialis tendon with a reflex hammer.
Brachioradialis: Position the patient with the arm supported. By cradling the elbow and draping the patient’s forearm over your arm, the brachioradialis muscle can be relaxed. The clinician taps the brachioradialis tendon with a reflex hammer.

Triceps: Position the client with the triceps muscle relaxed. The clinician taps the triceps tendon with a reflex hammer.
Patella: Position the client with the quadriceps & patella tendon relaxed. The clinician taps the patella tendon with a reflex hammer.

Medial Hamstring: Position the client with the semimembranosus tendon relaxed. The clinician taps the tendon with a reflex hammer.

Lateral Hamstring: Position the client with the biceps femoris relaxed. The clinician taps the biceps femoris tendon with a reflex hammer.

Achilles: Position the client with the gastroc/soleus & Achilles tendon relaxed. The clinician taps the Achilles tendon with a reflex hammer.
Tibialis Posterior: Position the client with the tibialis posterior tendon relaxed. The clinician taps the tibialis posterior tendon with a reflex hammer.
Jendrassik maneuver may be utilized if there is difficulty eliciting a reflexive response. The maneuver involves having the patient clench the teeth, flex fingers of both hands into a hook-like position, and interlocking the fingers together.
More cutting edge orthopedic information can be found in iOrtho+ Premium Mobile App. Subscribe for the low annual rate of only $9.99. If you prefer to just try iOrtho+ Premium for just 1 month, you can do so for just $1.99 Please visit https://iortho.xyz/ Prior blog posts are also available at https://iortho.xyz/
- Gulick DT. iOrtho+ Premium Web App. DTG Enterprises LLC. 2024
- Gulick, DT. OrthoNotes, 5th FA Davis Publishing, Philadelphia. 2023
- Lauder TD, et al. Predicting electrodiagnostic outcome in patients with upper-limb symptoms: Are history & physical examination helpful? Archives of Physical Medicine & Rehabilitation. 2000;81:436-441
- Magee D. Orthopedic Physical Assessment. 5th ed. Philadelphia, PA: WB Saunders Company; 2008.
- Teitelbaum JS, Eliasziw M, Garner M. Tests of Motor Function in Patients Suspected of having Mild Unilateral Cerebral Lesions. Canadian Journal of Neurological Science. 2002;29:337-344
- Wainner RS, Fritz JM, Irrgang JJ, et al. Reliability & diagnostic accuracy of the clinical examination & patient self- report measures for cervical radiculopathy. Spine 2003;28:52– 62.