

Functional Lower Extremity Tests
Clinicians have been known to struggle, on occasion, with the criteria for an individual to safely return to activity after an injury. What tests are the best ones to use? Are there are statistics to confirm the value of a test? Do normalize values exist for the population you are testing? All of these questions have very limited answers.
This blog will share 6 lower extremity functional tests to assess strength, symmetry, balance, and/or agility. The tests selected do not require any expensive equipment to perform. The tests described are:
 Hop for Distance Test is performed by standing on 1 leg and hopping as far as possible onto same leg. The patient must “stick” the landing for the hop to be scored/measured. The task should be repeated 3 times on each leg with the average distances used for comparison. If the involved leg distance is less than 85% of uninvolved leg, the test is deemed positive. There is also a significant correlation between the Hop for Distance Test and isokinetic knee extension peak torque production at 240°/second.
Hop for Distance Test is performed by standing on 1 leg and hopping as far as possible onto same leg. The patient must “stick” the landing for the hop to be scored/measured. The task should be repeated 3 times on each leg with the average distances used for comparison. If the involved leg distance is less than 85% of uninvolved leg, the test is deemed positive. There is also a significant correlation between the Hop for Distance Test and isokinetic knee extension peak torque production at 240°/second.

 Crossover Hop Test requires a straight line to be marked on the floor. The patient starts standing on 1 leg on 1-side of the line. The patient performs 3 hops with the same leg with each hop landing on the other side of the line. In other words, start to the right of the line and hop to the left, to the right, and to the left again. Each hop should be as far forward as possible. The task is repeated 3 times on each leg with the average the distances used for comparison. The patient should not touch the other foot down on the ground or land on the line for an effort to be scored/measured. If the involved leg distance is less than 85% of uninvolved leg, the test is deemed positive. Like the Hop for Distance Test, the Cross-over Hop Test has been correlated with isokinetic knee peak torque performance at the following velocities:
Crossover Hop Test requires a straight line to be marked on the floor. The patient starts standing on 1 leg on 1-side of the line. The patient performs 3 hops with the same leg with each hop landing on the other side of the line. In other words, start to the right of the line and hop to the left, to the right, and to the left again. Each hop should be as far forward as possible. The task is repeated 3 times on each leg with the average the distances used for comparison. The patient should not touch the other foot down on the ground or land on the line for an effort to be scored/measured. If the involved leg distance is less than 85% of uninvolved leg, the test is deemed positive. Like the Hop for Distance Test, the Cross-over Hop Test has been correlated with isokinetic knee peak torque performance at the following velocities:
-
-
-
-
-
-
-
-
-
- at 180°/sec = 0.69
- at 300°/sec = 0.64
- at 450°/sec = 0.53
-
-
-
-
-
-
-
-
Maximal Controlled Leap Test has the patient stand on 1-foot with his/her hands on the hips. The patient “leaps forward” as far as possible to land on the contralateral foot. The patient must “stick” the landing for the task to be scored/measured. The task should be repeated 3 times on each leg with the average distances used for comparison. If the involved leg distance is less than 85% of uninvolved leg, the test is deemed positive.
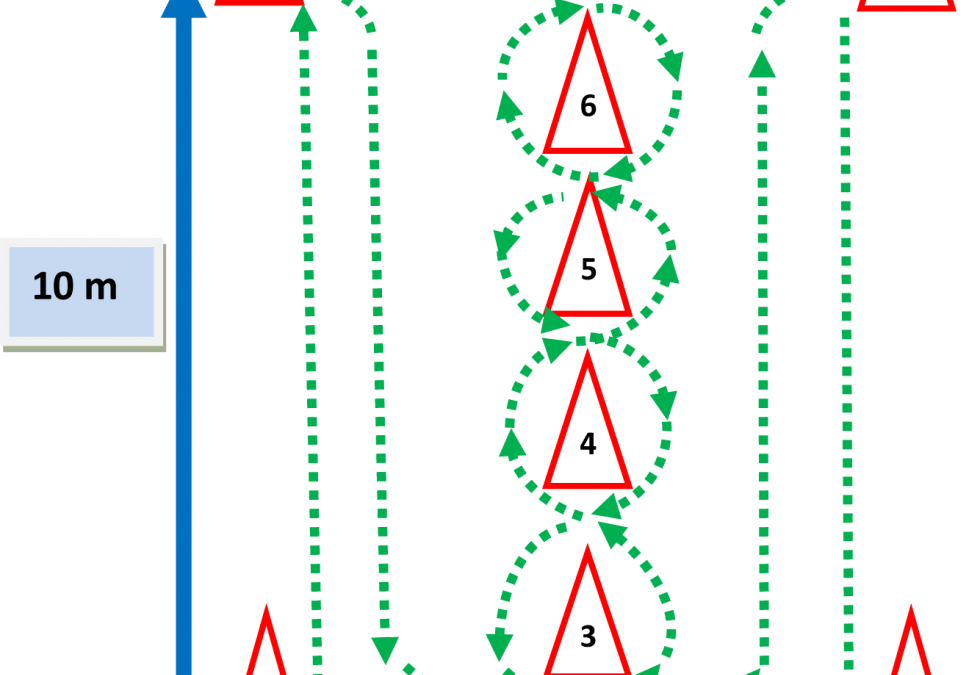
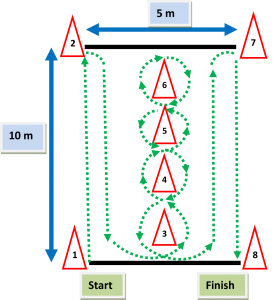 Illinois Agility Test requires the set-up of 8 cones as displayed in the diagram. The sequence of the test requires the patient to:
Illinois Agility Test requires the set-up of 8 cones as displayed in the diagram. The sequence of the test requires the patient to:
- start at cone “1”
- run 10 meters to cone “2”
- run 10 meters to cone “3”
- weave around cones “3, 4, 5, and 6” and back through “5, 4, and 3”
- run 5 meters to cone “7”
- and finally 5 meters to cone “8”
The ratings for this test are gender specific: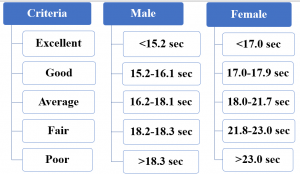
T-Test also requires a course set-up. In this case, 4 cones are places in the shape of a “T.” The patient will: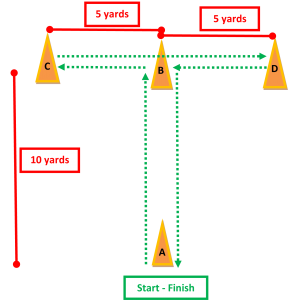
- start at cone “A”
- run 5 yards forward to cone “B”
- touch the base of cone “B” with the right hand
- shuffle left 5 yards & touch the base of cone “C” with left hand
- shuffle right 10 yards & touch the base of cone “D” with right hand
- shuffle left 5 yards & touch the base of cone “B”
- then back pedal past the starting point at cone “A”
The time is recorded from the start to the finish. There are no standards for this test and obviously no right to left comparisons. The best comparison is pre- and post-injury assessment but that requires the forethought of doing pre-season testing to have this data available.
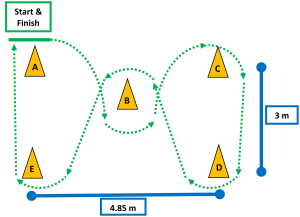 Zig Zag Run Test involves the set up of 5 cones as displayed. Again, the sequence of the task is specific. The patient:
Zig Zag Run Test involves the set up of 5 cones as displayed. Again, the sequence of the task is specific. The patient:
- starts at cone “A”
- zig zags around the cones in the following order “B – C – D – B – E – A”
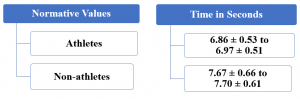
The run does not require the patient to touch the cones with his/her hand or foot. Although there are normative values provided for this test, they are not sport specific nor gender specific. Like the Zig Zag Run, the comparison would need to be pre- versus post-injury to be applied to a given individual.
Normative values are only one set of metrics for a given test. Sensitivity, specificity, and reliability are also important. The following table provides details on each of tests:
| Test | Statistical Data |
| Hop for Distance Test | Sensitivity = 38-58%
Specificity = 98% ICC uninjured = 0.88 – 0.96 ICC ACL reconstruction = 0.80 – 0.92 |
| Crossover Hop Test | ICC uninjured = 0.85 – 0.96
ICC ACL reconstructed = 0.84 – 0.98 |
| Maximal Controlled Leap Test | No statistical data reported |
| Illinois Agility Test | No statistical data reported |
| T-Test | ICC = 0.94-0.98 |
| Zig Zag Run Test | Inter-tester ICC: athletes = 0.97, non-athletes = 0.97
Intra-tester ICC: athletes = 0.92, non-athletes = 0.94 |
In summary, these tests are a few of many tests available to assess strength, symmetry, balance, and/or agility. The paucity of data is understandable given the number of possible combinations for gender and sports. The best scenario is to have pre-season data to which to compare. When that is not available, the next best thing could be comparison to another individual who plays the same position in a sport or performs a similar task. Granted that is not ideal but it could be better than no data at all.
For more cutting edge orthopedic information, subscribe to iOrtho+ Premium Mobile Web App, at https://iortho.xyz/
- Ageberg E, Zatterstrom R, Mortiz U: Stabiliometry and one leg hop test have high test-retest reliability, Scand J Med Sci Sports. 1998; 8:198-202
- Bandy WD, Rusche KR, Tekulve FY: Reliability and limb symmetry for five unilateral functional tests for the lower extremities, Isokinetics Exerc Sci. 1994; 4:108-111
- Barber SD, Noyes FR, Mangine RE et al: Quantitative assessment of functional limitations in normal and anterior cruciate ligament-deficient knees, Clin Orthop 1990; 255:204-214
- Bolgla LA, Keskula DR: Reliability of lower extremity functional performance test, J Orthop Sports Phys Ther. 1997; 26:138-142
- Brosky JA, Nitz AJ, Malone TR et al: Intrarater reliability of selected clinical outcome measures following anterior cruciate ligament reconstruction, J Orthop Sports Phys Ther 1999;29(1):39-48
- Clark NC, Gumbrell CJ, Rana S et al: Intratester reliability and measurement error of the adapted crossover hop for distance, Phys Ther Sport. 2002; 3:143-151
- Fry AC, Kraemer WJ, Weseman CA, et al. The effects of an off-season strength and conditioning program on starters and non-starters in women’s intercollegiate volleyball. Journal of Applied Sports, Science, and Research. 1991;5:174-181
- Greenberger H, Paterno MV. Relationship of Knee Extensor Strength and Hopping Test Performance in the Assessment of Lower Extremity Function. JOSPT. 1995;22(5):202-206.
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Harman E, Garhammer J, Pandorf C. Administration, scoring, & interpretation of selected tests. In: Baechle TR, Earle RW (eds). Essentials of Strength & Conditioning. Champaign, IL: Human Kinetics, 2000
- Hoffman J. Norms for Fitness, Performance, & Health. Champaign, IL: Human Kinetics, 2006
- Hopper DM, Goh SC, Wentworth LA et al: Test-retest reliability of knee rating scales and functional hop tests one year following anterior cruciate ligament reconstruction, Phys Ther Sport. 2002; 3:10-18
- Juris PM, Phillips EM, Dalpe C et al: A dynamic test of lower extremity function following anterior cruciate ligament reconstruction and rehabilitation, J Orthop Sports Phys Ther. 1997; 26:184-191
- Kramer JF, Nusca D, Fowler P et al: Test-retest reliability of the one-leg hop test following ACL reconstruction, Clin J Sport Med. 1992; 2:240-243
- Myer GD, Schmitt LC, Brent JL, Ford KR, Barber Foss KD, Scherer BJ, Heidt Jr RS, Divine JG, Hewett TE. Utilization of Modified NFL Combine Testing to Identify Functional Deficits in Athletes Following ACL Reconstruction. JOSPT, 2011; 41(6):377–387
- Noyes FR, Barber SD, Mangine RE: Abnormal lower limb symmetry determined by functional hop tests after anterior cruciate rupture, Am J Sports Med. 1991; 19:513-518
- Ortiz A, Olson SL, Roddey TS, Morales J. Reliability of selected physical performance tests in young adult women. Journal of Strength & Conditioning Research. 2005;19:39-44
- Paterno MV, Greenberger HB: The test-retest reliability of a one legged hop for distance in young adults with and without ACL reconstruction, Isokinetics Exerc Sci. 1996;6:1-6
- Pauole K, Madole K, Garhammer J, Lacourse M, Rozenek R. Reliability and validity of the T-test as a measure of agility, leg power, and leg speed in college-aged men and women. Journal of Strength and Conditioning Research. 2000;14:443-450
- Petschnig R, Baron R, Albrecht M. The relationship between isokinetic quadriceps strength test & hop tests for distance & one-legged vertical jump test following anterior cruciate ligament reconstruction. 1998;28(1):23-31
- Risberg MA, Ekeland A: Assessment of functional tests after anterior cruciate ligament surgery, J Orthop Sports Phys Ther 19:212-217, 1994.
- Reiman MP, Manske RC. Functional Testing in Human Performance. Champaign, IL: Human Kinetics, 2009
- Ross MD, Langford B, Wheland PJ: Test-retest reliability of 4 single leg horizontal hop tests, J Strength Cond Res. 2002; 16:617-622
- Seminick D. Tests and measurements: The T-test. NSCA Journal. 1990;12:36-37
- Strobel M, Stedtfeld HW: Diagnostic evaluation of the knee, Berlin, Springer-Verlag. 1990
- Tegner Y, Lysholm J, Lysholm M, Gillquist J. A performance test to monitor rehabilitation & evaluate anterior cruciate ligament injuries. American Journal of Sports Medicine. 1986;14:156-159
- Wilk KE, Romaniello WT, Soscia SM, Arrigo CA, Andrews JR. The relationship between subjective knee score, isokinetic testing & functional testing of the ACL reconstructed knee. JOSPT. 1994;20(2):60-73