


The Value of Clustering Carpal Tunnel Tests
Carpal Tunnel Anatomy
The carpal tunnel is an osteofibrous canal of the wrist. It is defined by the boundaries of the carpal bones and the flexor retinaculum. Within the carpal tunnel are nine tendons and the median nerve. The latter being a significant structure since one of the hallmark signs is edema which puts a back-pressure on the median nerve to produce burning, tingling, and numbness into the palm, thumb, and/or index and middle fingers. Individuals with diabetes, hypertension, high sodium intake, sedentary lifestyles, smoking, and high body mass index (BMI) have as increased risk of carpal tunnel syndrome (CTS).
Clinical Predictor Rules
Research by Wainner et al (2005) and Childs and Cleland (2006) have contributed to the development of Carpal Tunnel Clinical Predictor Rules. The following are the parameters identified as the clinical predictors:
- Flick Test relieves symptoms (discussed below)
- Wrist ratio (Anterior-Posterior width / Medial-Lateral width) > 0.67
- Symptoms Severity Scale > 1.9
- Diminished sensation of thenar eminence
- Age > 45 years old
The likelihood of having CTS is influenced by the number of the signs/symptoms present. As one can see, the more positive tests, the greater the likelihood of a diagnosis of CTS.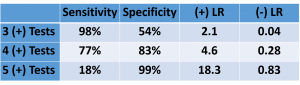
Carpal Tunnel Clinical Tests
There are at least 5 carpal tunnel tests in the literature. We will discuss the performance of these tests, the metrics, and the influence of clustering various tests. These tests include: Phalens, Reverse Phalens, Flick, Carpal Tunnel Compression, and Tinel sign.
Phalen & Reverse Phalen Test 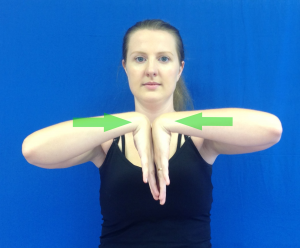
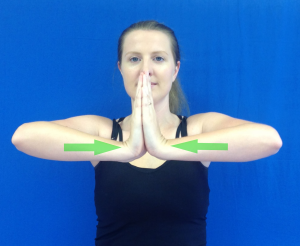
These tests aim to compress the median nerve in the carpal tunnel with endrange flexion or extension, respectively. For the Phalen test, the patient puts the back of both hands together with his/her arms elevated at the level of the shoulder. For the Reverse Phalen test, the patient puts the palms together with his/her arms elevated at the level of the shoulder. An easy way to remember the positions for these two tests is: Phalen Test by ‘Fingers-Falling.’ In contrast, the Reverse Phalen is “fingers Rising.” A positive test is numbness or tingling into the median nerve distribution, i.e. palmar surface of digits 1, 2, and 3.
Flick Maneuver
The Flick Maneuver is an interesting test. It does exactly what is sound like…..it involves flicking the wrist. Where most tests look to reproduce the symptoms, this test is positive when the symptoms (paresthesias into the median nerve distribution) subside as a result of the repeated flicking maneuver of the wrist. As per the summary statistical chart below, sensitivity and specificity have a wide range. This may be due to the interpretation of the magnitude of the symptom relief being highly variable.
 Carpal Tunnel Compression Test
Carpal Tunnel Compression Test
The carpal tunnel compression test simply involves positioning the wrist in at least 60° of flexion and maintaining the position for 30 seconds. This position is essentially the same as a Phalen test without addressing the position of the shoulder. A positive test is numbness or tingling into the median nerve distribution. Thus, it is not a surprise to learn the statistics are almost exactly the same as the Phalen test.
Tinel Sign
A Tinel sign is a common sign used in a variety of locations of the body and indicates that a nerve is irritated. This test can be performed at the elbow, shoulder, ankle, and wrist. A Tinel sign is positive when light percussing over the nerve elicits tingling into the distribution of the nerve. When performing this test on the wrist, one taps over the anterior aspect of the wrist to incriminate the median nerve.
The statistics for this individual test is highly variable. This may be attributed to the interpretation of the magnitude of the paresthesias produced. However, when coupled with the Phalen test or Flick maneuver, the diagnostic metric improves.
CTS Test Statistics
When assessing the results of a test, it is always helpful when you have a contralateral structure to which you can compare. Obviously it is always desirable to obtain positive results from at least two tests for a given tissue to provide some reassurance of the diagnosis. Notwithstanding the high variability of the statistical data for the individual tests, there is slightly better data with the clustering of carpal tunnel tests. The chart below displays these results.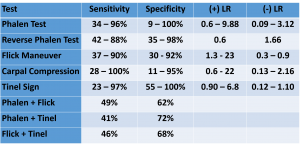
For videos of the CTS tests and more cutting edge orthopedic information in iOrtho+ Premium Mobile App, please visit https://iortho.xyz/
- Ahn D. Hand Elevation: A new test for carpal tunnel syndrome. Annuals of Plastic Surgery. 2001;46:120-124
- Amirfeyz B, Gozzard C, Leslie IJ. Hand elevation test for assessment of carpal tunnel syndrome. Journal of Hand Surgery. 2005;30B(4):361-364
- Bruske J, Bednarski M, Grzelee H, Zyluk A. The usefulness of Phalen Test & the Hoffman-Tinel sign in the diagnosis of carpal tunnel syndrome. Acta Orthopaedica Belgica. 2002;68(2):141-150
- Childs JD, Cleland JA. Development and application of clinical predictor rules to improve clinical decision making in physical therapy practice. Physical Therapy. 2006;122-131
- deKrom MC, Knipschild PG, Kester AD, Spaans F. Efficacy of provocative tests for diagnosis of carpal tunnel syndrome. Lancet. 1990;335(8686):393-395
- Durkan JA. The carpal compression test: an instrumented device for diagnosing carpal tunnel syndrome. Orthopedic Review. 1994;23:522-525
- El Miedany Y, Ashour S, Youssef S, et al. Clinical diagnosis of carpal tunnel syndrome: old tests-new concepts. Joint Bone & Spine. 2008;75:451-457
- Fertl E, Wober C, Zeithofer J. The serial use of 2 provocative tests in the clinical diagnosis of carpal tunnel syndrome. Acta Neurology Scandanavia. 1998;98:328-332
- Gonzalez del Pinto, et al. Value of the carpal compression test in the diagnosis of carpal tunnel syndrome. Journal Hand Surgery British. 1997;22:38-41
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC, 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia, 2018
- Gunnarsson LG, Amilon A, Hellstrand P, Leissner P, Philipson L. The diagnosis of carpal tunnel syndrome. Sensitivity & specificity of some clinical & electrophysiological tests. Journal Hand Surgery. 1997;22:34-37
- Hansen P, Mickelsen P, Robinson L. Clinical utility of the flick maneuver in diagnosing carpal tunnel syndrome. American Journal of Physical Medicine & Rehabilitation. 2004;83:363-367
- Heller L, Ring H, Costeff H, Solzi P. Evaluation of Tinel’s & Phalen’s signs in diagnosis of the carpal tunnel syndrome. European Neurology. 1986;25(1):40-42
- Johnson E, Gatens T, Pointdexter D, Bowers D. Wrist dimension: correlation with median sensory latencies. Archive of Physical Medicine and Rehabilitation. 1993;64:556-557
- Katz J, Larson M, Sabra A, et al. The carpal tunnel syndrome: diagnosis utility of the history & physical examination findings. Annals International Medicine. 1990;112:321-327
- Kaul MP, Pagel KJ, Wheatley MJ, Dryden JD.. Carpal compression test & pressure provocation test in veterans with median-distribution paresthesias. Muscle Nerve. 2001;24:107-111
- Krendel DA, Jobsis M, Gaskell Jr PC, & Sanders DB. The flick sign in carpal tunnel syndrome. Journal Neurology Neurosurgery Psychiatry. 1986 February; 49(2): 220-221
- Kuhlman KA, Hennessey WJ. Sensitivity & specificity of carpal tunnel syndrome signs. American Journal of Physical Medicine & Rehabilitation. 1997;76:451-457
- LaJoie AS, McCabe SJ, Thomas B, Edgell SE. Determining the sensitivity & specificity of common diagnostic tests for carpal tunnel syndrome using latent class analysis. Plastic Reconstructive Surgery. 2005;116:502-507
- LaStayo P, Howell J. Clinical provocative tests used in evaluating wrist pain: a descriptive study. Journal Hand Therapy. 1995;8:10-17
- Marx RG, Bombardier C, Wright JC. What do we know about the reliability & validity of physical examination tests used to examine the upper extremity? Journal of Hand Surgery. 1999;24A:185-193
- Moldaver J: Tinel sign: Its characteristics & significance, Journal Bone Joint Surgery American 1978;60:412-414
- Pryse-Phillips WE. Validation of a diagnostic sign in carpal tunnel syndrome. Journal Neurology Neurosurgery Psychiatry. 1984 Aug;47(8):870-872
- Szabo RM, Slater RR. Diagnostic testing in carpal tunnel syndrome. Journal of Hand Surgery. 2000;25(1):184
- Tetro AM, Evanoff BA, Hollstien SB, Gelberman RH. A new provocation test for carpal tunnel syndrome. Assessment of wrist flexion & nerve compression. Journal Bone & Joint Surgery. 1998;80:493-498
- Wainner R, Fritz J, Irrgang J, Delitto A, Allison S, Boninger M. Development of a clinical predictor rule for the diagnosis of carpal tunnel syndrome. Archives of Physical Medicine. 2005;86:609-618