

Subscapularis: How is the Largest RC Muscle so Overlooked?
Subscapularis Anatomy
The subscapularis muscle originates from the subscapular fossa and goes through the axilla to attach to the lesser tubercle of the humerus. Tendinous fibers have been reported to extend to the greater tubercle with insertions into the bicipital groove. The subscapularis is the only one of the four rotator cuff muscles that functions as an internal rotator. It also serves as an adductor and plays an important role in keeping the humerus in the glenoid fossa. As the largest and strongest cuff muscle, tihe subscapularis is estimated to provide 53% of total cuff strength.
Mechanism of Injury
The mechanism of subscapularis injury is over extension of the arm or secondary to shoulder impingement. However, the subscapularis is also subjected to age-related degeneration. There are several clinical tests to assess the subscapularis, five of which are fairly well researched: Internal Rotation (IR) Lag sign, Lift-off test, Belly press, Belly-off, and Bear hug. All of the test incorporate IR of the shoulder but some are active tests and others are resistive tests. The one feature the clinician must be aware of is the challenge of some of the testing positions. If an individual cannot assume a testing position, a decision regarding the (+) or (-) outcome of the test cannot be rendered.
Subscapularis Tests
 For the IR Lag sign, the clinician stands behind the seated patient and places the affected arm behind the back. The clinician controls the patient’s arm at the elbow and wrist to place the arm in ~20-30° of extension and the forearm/hand behind the back. The patient is told to hold the arm in that position as clinician releases the wrist contact (maintain elbow contact). A (+) test is the forearm drops towards the back, i.e. into ER due to the inability to maintain IR. A partial tear may only result in a slight lag (5°), while the larger the lag the larger the tear.
For the IR Lag sign, the clinician stands behind the seated patient and places the affected arm behind the back. The clinician controls the patient’s arm at the elbow and wrist to place the arm in ~20-30° of extension and the forearm/hand behind the back. The patient is told to hold the arm in that position as clinician releases the wrist contact (maintain elbow contact). A (+) test is the forearm drops towards the back, i.e. into ER due to the inability to maintain IR. A partial tear may only result in a slight lag (5°), while the larger the lag the larger the tear.
 The lift-off test, AKA Gerber test, is also performed in the seated position, with the hand of the involved shoulder in the curve of the lumbar spine. The patient is asked to lift the hand off the back and maintain the IR position against resistance. A (+) test is the reproduction of pain and/or weakness or the inability to lift hand off back. This test has been identified as one that is best for detecting larger tears (>75% of the subscapularis).
The lift-off test, AKA Gerber test, is also performed in the seated position, with the hand of the involved shoulder in the curve of the lumbar spine. The patient is asked to lift the hand off the back and maintain the IR position against resistance. A (+) test is the reproduction of pain and/or weakness or the inability to lift hand off back. This test has been identified as one that is best for detecting larger tears (>75% of the subscapularis).
As mentioned previously, if the position cannot be assumed, you can’t render a decision on the test. Fortunately, there are other options for testing the subscapularis if the position cannot be assumed. Both the belly press and belly off test use resisted IR with the hand of the involved shoulder on the belly.
 The belly press test, AKA Napolean sign, is in the seated position with the hand on the belly. The patient is asked to press the hand into the belly. Reproduction of pain and/or inability to IR is a (+) test. Inability to perform IR may result in substitution with shoulder extension or wrist flexion. Stabilizing the elbow may help prevent this, or at least cue th
The belly press test, AKA Napolean sign, is in the seated position with the hand on the belly. The patient is asked to press the hand into the belly. Reproduction of pain and/or inability to IR is a (+) test. Inability to perform IR may result in substitution with shoulder extension or wrist flexion. Stabilizing the elbow may help prevent this, or at least cue th e clinician into the compensatory motion. The belly press test has been reported to require tears >50% to be positive. Another option is to perform the test is supine where the shoulder is blocked from going into extension. By moving to the supine position the Belly Press begins to look like the belly off test.
e clinician into the compensatory motion. The belly press test has been reported to require tears >50% to be positive. Another option is to perform the test is supine where the shoulder is blocked from going into extension. By moving to the supine position the Belly Press begins to look like the belly off test.
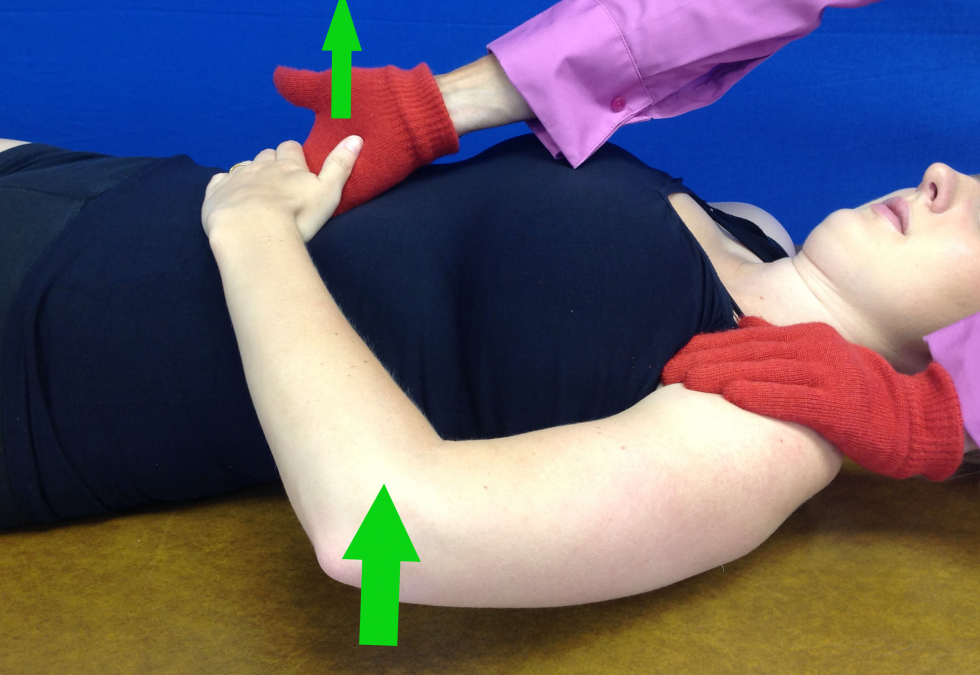
 The belly-off test assumes the same position as the belly press test, but in this test instead of the patient pushing the hand into the belly to perform shoulder IR, the clinician tries to pull the patient’s hand off of the belly (pulling into ER). Reproduction of pain and/or inability to IR is a (+) test. The same concerns are present for substitution of the testing task for the belly off as the belly press.
The belly-off test assumes the same position as the belly press test, but in this test instead of the patient pushing the hand into the belly to perform shoulder IR, the clinician tries to pull the patient’s hand off of the belly (pulling into ER). Reproduction of pain and/or inability to IR is a (+) test. The same concerns are present for substitution of the testing task for the belly off as the belly press.
 The bear hug is the newest of the subscapularis tests. This test can be performed in sitting with the palm of the involved shoulder on the opposite shoulder. The elbow is in front of body elevated to 90° to assess the lower subscapularis fibers and positioned at 45° of elevation to assess the upper subscapularis fibers. In order words, the arm is high for the inferior fibers and low for the superior fibers. In the respective position, the clinician resists IR by attempting to pull the hand off the shoulder. As for test interpretation, inability to hold the hand against the opposite shoulder or weakness >20% of contralateral arm would be considered a (+) test. This test has been reported to be capable of detecting tears as small as 30%. This is the only subscapularis test that differentiates the upper and lower fibers. Does that really matter to a clinician? Unless you’re a surgeon, it probably does not make a difference, but it may be helpful in developing therapeutic exercise programs.
The bear hug is the newest of the subscapularis tests. This test can be performed in sitting with the palm of the involved shoulder on the opposite shoulder. The elbow is in front of body elevated to 90° to assess the lower subscapularis fibers and positioned at 45° of elevation to assess the upper subscapularis fibers. In order words, the arm is high for the inferior fibers and low for the superior fibers. In the respective position, the clinician resists IR by attempting to pull the hand off the shoulder. As for test interpretation, inability to hold the hand against the opposite shoulder or weakness >20% of contralateral arm would be considered a (+) test. This test has been reported to be capable of detecting tears as small as 30%. This is the only subscapularis test that differentiates the upper and lower fibers. Does that really matter to a clinician? Unless you’re a surgeon, it probably does not make a difference, but it may be helpful in developing therapeutic exercise programs.
Subscapularis Statistics
To summarize the subscapularis tests, there are two in which the involved hand is placed on the lumbar spine. One test involves an isometric contraction (IR lag) and the other a concentric contraction (lift off). There are also two tests that place the involved hand on the belly. One test is concentrically active (belly press) and the other is an eccentric motion (belly off). Finally, there is the bear hug, which places the involved hand on the opposite shoulder and IR is resisted at 90° and 45° of elevation. The table below summarizes the statistical data associated with clinical decision-making. Four of the five tests have high specificity, indicating they are strong diagnostic tools. All of the tests are good screening tool for full thickness (FT) tears but that is not the case for partial thickness (PT) tears. As is the case for any pathology, the clinician should look for (+) results in more than one test for a subscapularis diagnosis.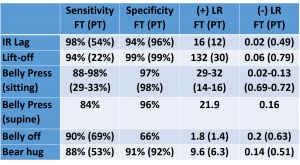
For more cutting edge orthopedic information in the iOrtho+ Premium Mobile App, please visit https://iortho.xyz/
- Alqunaee M, Galvin R, Fahey T. Diagnostic accuracy of clinical tests for subacromial impingement syndrome: A systematic review & meta-analysis. Archive of Physical Medicine & Rehabilitation. 2012;93:229-236
- Bak K, Sorensen AKB, Jorgensen U, Nygaard M, Krarup AL, Thune C, Sloth C, Pedersen ST. The value of clinical tests in acute full-thickness tears of the supraspinatus tendon: Does subacromial lidocaine injection help in clinical diagnosis? Arthroscopy. 2010;26(6);734-742
- Barth JRH, Burkhart SS, DeBeer JF. Bear-Hug Test: A new & sensitive test for diagnosing a subscapular tear. Arthroscopy: Journal of Arthroscopy & Related Surgery. October 2006;22(10):1076-1084
- Chao S, Thomas S, Yucha D, Kelly JD, Driban J, Swanik K. An electromyographic assessment of the bear hug: an examination for the evaluation of the subscapularis muscle. Arthroscopy. 2008;24(11):1265-1270
- Chao S, Yucha D, Kelly JD. An electromyographic assessment of the bear-hug. An exam for the evaluation of the subscapularis. Paper #458. Presented at the American Academy of Orthopaedic Surgeons 76th Annual Meeting. Feb. 25-27, 2009. Las Vegas
- Fowler EM, Horsley IG,Rolf CG. Clinical & arthroscopic findings in recreationally active patients. Sports Medicine, Arthroscopy, Rehabilitation, Therapy, & Technology. 2010;2:2-8
- Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle, Journal Bone Joint Surgery British 1991;73:389-394
- Greis PE, Kuhn JE, Schultheis J et al: Validation of the lift-off sign test & analysis of subscapularis activity during maximal internal rotation, American Journal Sports Medicine 1996;24:589-593
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Hertel R, Ballmer FT, Lambert SM, Gerber CH. Lag signs in the diagnostic of rotator cuff rupture. Journal of Shoulder & Elbow Surgery. 1996;5(4):307-313
- Lyons RP, Green A: Subscapularis tendon tears, Journal American Academy Orthopedic Surgery 2005;13:353-363
- McClusky CM: Classification & diagnosis of glenohumeral instability in athletes, Sports Medicine Arthroscopic Reviews 2000;8:158-169
- Miller CA, Forrester GA, Lewis JS. The validity of the lag signs in diagnosing full-thickness tears of the rotator cuff: a preliminary investigation. Archives Physical Medicine Rehabilitation. 2008;89(6):1162-1168
- Ostor AJ, Richards CA, Prevost AT, Hazleman BL, Speed CA. Interrater reproducibility of clinical tests for rotator cuff lesions. Annals Rheumatic Disease. 2004;63:1288-1292
- Rigsby R, Sitler M, Kelly JD. Subscapularis tendon integrity: an examination of shoulder index tests. Journal of Athletic Training. 2010;45(4):404-406
- Scheibel M, Magosch P, Pritsch M, Lichtenberg S. The belly-off sign: A new clinical diagnostic sign for subscapularis lesions. Arthroscopy. 2005;21(10):1229-1235
- Takeda Y, Fujii K, Miyatake K, Kawasaki Y, Nakayama T, & Sugiura K. Diagnostic value of the supine Napolean test for subscapularis tendon lesions. Arthroscopy: the Journal of Arthroscopic & related Surgery. 2016 June 24
- Ticker JB, Warner JJ: Single-tendon tears of the rotator cuff: Evaluation & treatment of subscapularis tears, Orthopedic Clinical North American 1997;28:99-116
- Tokish JM, Decker MJ, Ellis HB, Torry MR, Hawkins RJ. The belly-press test for the physical examination of the subscapularis muscle: electromyographic validation & comparison to the lift-off test. Journal of Shoulder & Elbow Surgery. 2003;12(5):427-430