
The Elbow is Connected to the Wrist Bone!


In comparison with other joints of the body, the elbow has very few clinical tests. Aside from manual muscle testing, all of the elbow tests focus on the two collateral ligaments, the tendon attachments to the epicondyles, and the ulnar nerve. There is also limited data on sensitivity and specificity for the elbow tests.
However, before embarking on the elbow tests, one should be sure to screen the cervical spine and shoulder. This includes neural tension tests. Getting a patient history and a mechanism of injury are also important. Listening to the patient about the type, magnitude, duration of the pain. This often helps identify the source of the pathology.
Collateral Ligaments
 Let’s start with testing the collateral ligaments: the lateral/radial and medial/ulnar collateral ligaments. The lateral collateral ligament is assessed via a varus stress. With the elbow slightly flexed and the humerus stabilized proximal to elbow, the forearm is grasped distally, and a varus force is applied perpendicular to the joint line (note: the alignment of the forearm with the desired direction of force). One might opt to place the patient’s distal arm under your arm between the humerus and your rib cage. This frees up a hand to palpate the joint line. Testing can also be done in prone to enhance the stabilization of the arm. A positive test is pain or joint gapping/instability as compared to the contralateral elbow.
Let’s start with testing the collateral ligaments: the lateral/radial and medial/ulnar collateral ligaments. The lateral collateral ligament is assessed via a varus stress. With the elbow slightly flexed and the humerus stabilized proximal to elbow, the forearm is grasped distally, and a varus force is applied perpendicular to the joint line (note: the alignment of the forearm with the desired direction of force). One might opt to place the patient’s distal arm under your arm between the humerus and your rib cage. This frees up a hand to palpate the joint line. Testing can also be done in prone to enhance the stabilization of the arm. A positive test is pain or joint gapping/instability as compared to the contralateral elbow.
 The medial collateral ligament of the elbow is assessed with a valgus stress to the elbow. With the elbow slightly flexed and the humerus stabilized proximal to the elbow, the forearm is grasped distally, and a valgus force is imparted perpendicular to the joint line. Pain along the collateral ligament or joint gapping/instability is a positive test.
The medial collateral ligament of the elbow is assessed with a valgus stress to the elbow. With the elbow slightly flexed and the humerus stabilized proximal to the elbow, the forearm is grasped distally, and a valgus force is imparted perpendicular to the joint line. Pain along the collateral ligament or joint gapping/instability is a positive test.
 Neither the varus nor valgus stress tests have sensitivity or specificity values in the literature. In addition to the standard valgus stress, the Moving Valgus test also challenges the medial collateral ligament. This test was reported by O’Driscoll et al in 2002. The testing position requires the arm to be brought up into 90° of abduction, full ER, and full elbow flexion. A valgus force is applied to the elbow as it is quickly extended. If this produces pain in what is known as the “shear angle,” the test is positive. The “shear angle” is the midrange of elbow flexion between 120° & 70° of motion. Sensitivity is 100%, meaning that if there is no indication of pain or discomfort within the shear angle, then you can confidently rule out injury to the medial collateral ligament. Specificity is modest (75%), meaning it is a respectable indicator of injury to the medial collateral ligament.
Neither the varus nor valgus stress tests have sensitivity or specificity values in the literature. In addition to the standard valgus stress, the Moving Valgus test also challenges the medial collateral ligament. This test was reported by O’Driscoll et al in 2002. The testing position requires the arm to be brought up into 90° of abduction, full ER, and full elbow flexion. A valgus force is applied to the elbow as it is quickly extended. If this produces pain in what is known as the “shear angle,” the test is positive. The “shear angle” is the midrange of elbow flexion between 120° & 70° of motion. Sensitivity is 100%, meaning that if there is no indication of pain or discomfort within the shear angle, then you can confidently rule out injury to the medial collateral ligament. Specificity is modest (75%), meaning it is a respectable indicator of injury to the medial collateral ligament.
Muscle of the Elbow & Forearm
Each of the epicondyles of the elbow serve as attachments for multiple tendons. Stressing these soft tissues can be done through resisting a muscle contraction or elongating the tissue via a passive stretch. The lateral epicondyle is the attachment for the wrist extensors and forearm supinators. The Cozen sign and Mill test are used to assess for lateral epicondylitis/osis. The Cozen sign resists muscle activation, while the Mill test places the same tissues on stretch.
 For the Cozen sign, the arm is relaxed at the side with the elbow flexed to 90° and the forearm pronated. The clinician resists supination and wrist extension. A positive test is pain at the lateral epicondyle or proximal musculotendinous junction of wrist extensors. The muscles most commonly involved in lateral epicondylitis are the extensor carpal radialis longus and brevis. The Cozen sign incriminates these muscles through an active
For the Cozen sign, the arm is relaxed at the side with the elbow flexed to 90° and the forearm pronated. The clinician resists supination and wrist extension. A positive test is pain at the lateral epicondyle or proximal musculotendinous junction of wrist extensors. The muscles most commonly involved in lateral epicondylitis are the extensor carpal radialis longus and brevis. The Cozen sign incriminates these muscles through an active contraction and/or resistance. Whereas, the Mill test attempts to reproduce the lateral epicondyle pain via elongation of the tissue. The arm is relaxed at the side with the elbow fully extended. The wrist is passively stretched into wrist flexion with forearm pronation. In isolating the extensor digitorum muscle, the Maudsley test can be used. The extensor digitorum is commonly involved in
contraction and/or resistance. Whereas, the Mill test attempts to reproduce the lateral epicondyle pain via elongation of the tissue. The arm is relaxed at the side with the elbow fully extended. The wrist is passively stretched into wrist flexion with forearm pronation. In isolating the extensor digitorum muscle, the Maudsley test can be used. The extensor digitorum is commonly involved in 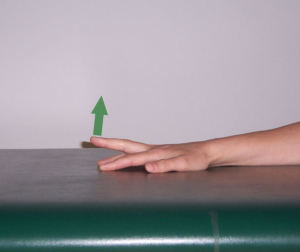 lateral epicondylitis/epicondylosis. To activate this muscle you would ask the patient to extend the third digit. If that fails to produce pain, resistance can be applied to increase the muscle activation. There are no data regarding sensitivity or specificity for any of these tests for the extensor mechanism.
lateral epicondylitis/epicondylosis. To activate this muscle you would ask the patient to extend the third digit. If that fails to produce pain, resistance can be applied to increase the muscle activation. There are no data regarding sensitivity or specificity for any of these tests for the extensor mechanism.
To assess the musculature off the medial epicondyle, i.e. wrist/finger flexors and forearm pronators, we can perform maneuvers that are the exact opposite of the Cozen sign and Mill test. Although there are no formal names for these tests, the clinical application of resisting and stretching these tissues makes sense. The arm is placed at the side with 90° of elbow flexion and the forearm supinated. Forearm pronation with wrist/finger flexion can be resisted to incriminate the contractile elements or the the wrist/fingers can be passively extended with forearm supination (to end range) to elongate the soft tissue originating from the medial epicondyle. Unfortunately, since no one has “claimed” these tests, there is no statistical data to report.
 Likewise the pronator teres arises from the medial epicondyle. The pronator teres test is used to assess for compression neuropathy of the median nerve at the anterior elbow. The clinician grasps the patient’s hand in a hand-shake position, i.e. elbow flexed, forearm half-way pronated, wrist neutral. Resistance is then applied to the pronators via the clinician’s attempt to supinate the patient’s forearm. Tenderness over the pronator teres muscle or pain &/or numbness into the first three fingers and palm would be a positive test. Weakness may also be present with flexion/abduction of the thumb.
Likewise the pronator teres arises from the medial epicondyle. The pronator teres test is used to assess for compression neuropathy of the median nerve at the anterior elbow. The clinician grasps the patient’s hand in a hand-shake position, i.e. elbow flexed, forearm half-way pronated, wrist neutral. Resistance is then applied to the pronators via the clinician’s attempt to supinate the patient’s forearm. Tenderness over the pronator teres muscle or pain &/or numbness into the first three fingers and palm would be a positive test. Weakness may also be present with flexion/abduction of the thumb.
Ulnar Nerve Assessment
Finally, we need to address the ulnar nerve. This structure passes through the cubital tunnel on the medial aspect of the elbow. The nerve is placed under stress when it is compressed or tensioned with elbow flexion. The pressure flexion test fulfills these criteria. When the patient is sitting with the elbow maximally flexed, the clinician will apply and maintain firm pressure just proximal to the cubital tunnel for 30 to 60 seconds. A positive test would be reproduction of neurologic symptom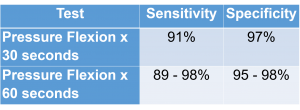 s along the ulnar nerve distribution – 4th and 5th digits. From the metrics, one can see it is of little value to hold this position for 60 seconds. The 30 second data is clearly sufficient in establishing a positive test.
s along the ulnar nerve distribution – 4th and 5th digits. From the metrics, one can see it is of little value to hold this position for 60 seconds. The 30 second data is clearly sufficient in establishing a positive test.
Summary
And that wraps up the elbow! Once again, there are not a whole lot of tests, and there is even less literature to support their use. Nonetheless, if one knows anatomy and the actions of the muscles, the performance of the various tests discussed here becomes rather intuitive. For more cutting edge orthopedic information in iOrtho+ Premium Mobile App, please visit the learning modules at https://iortho.xyz/
- Callaway GH, Field LD, Deng XH, et al. Biomechanical evaluation of the medial collateral ligament of the elbow. Journal of Bone and Joint Surgery. 1997;79(8):1223-1231
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC. 2020
- Gulick, DT. OrthoNotes, 4th FA Davis Publishing, Philadelphia. 2018
- Hartz CR, Linscheid CL, Gramse RR, Daube JR. The pronator teres syndrome: compressive neuropathy of the median nerve. The Journal of Bone and Joint Surgery (American) 1981;63(6): 885-890
- Magee D. Orthopedic Physical Assessment. 5th ed. Philadelphia, PA: WB Saunders Company; 2008.
- Morris HH, Peters BH. Pronator syndrome: clinical and electrophysiological features in seven cases. Journal of Neurology, Neurosurgery, and Psychiatry. 1976;39(5): 461-464.
- O’Driscoll SW, Lawton RM, Smith AM: The “moving valgus stress test” for medial collateral ligament tears of the elbow, American Journal Sports Medicine 2005;33:231-239
- O’Driscoll SW: Acute, recurrent & chronic elbow instabilities. In Norris TR, editor: Orthopedic knowledge update 2: shoulder & elbow, Rosemont, Ill, 2002, American Academy of Orthopedic Surgeons
- Regan WD, Morrey BF: The physical examination of the elbow. In Morrey BF, editor: The elbow & its disorders, Philadelphia, 1993, WB Saunders.
- Wertsch JJ, Melvin J. Median nerve anatomy and entrapment syndromes: a review. Archives of Physical Medicine and Rehabilitation. 1982;63(12):623-627