

Importance of Shoulder Palpation
Can you put 1 finger on the location of your pain? A question frequently used to identify the location of a patient’s pain. This can be a very helpful piece of information. From there, we typical move away from that location to screen out other possible tissues as we zone in on the location identified.
Palpation should be a performed in a systematic manner. The touch should be firm and intentional. “Creepy fingers” are not only ineffective but may make a patient feel uncomfortable. Several effective palpation techniques are modeled by a wonderful book known as the Trail Guide to the Body by Andrew Biel. 
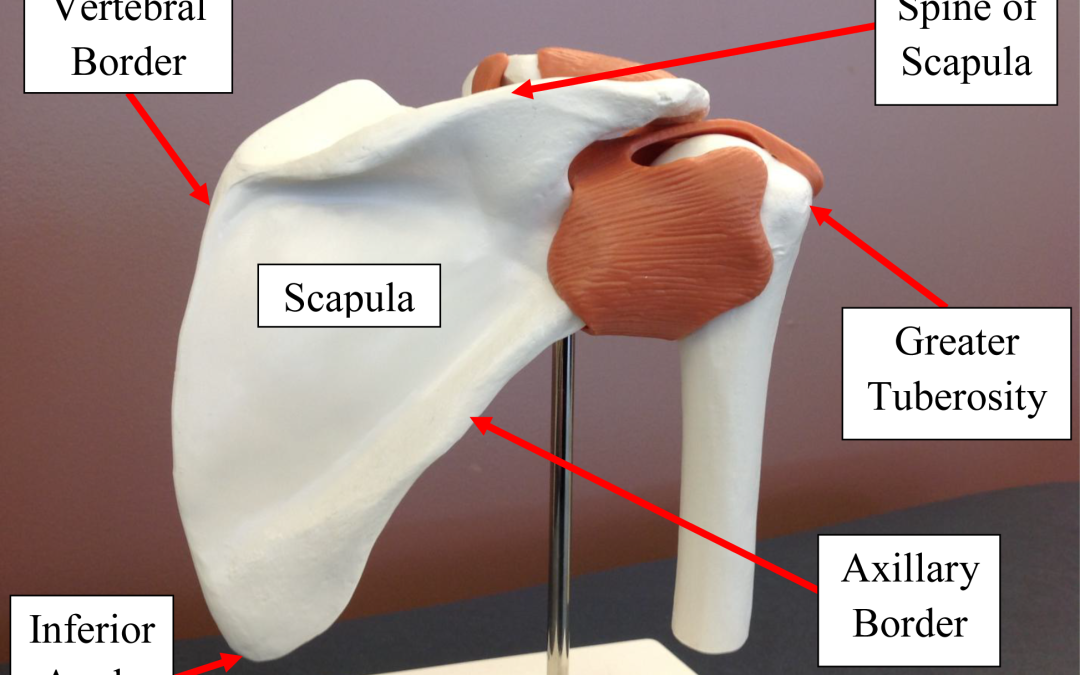
Using the approach that palpation is like following a trail of anatomical structures, let’s palpate the shoulder. Given that most individual’s report pain in or immediately around the glenohumeral joint line, starting with the scapula seems to make sense. Starting at the inferior angle of the scapula allows you to identify the orientation of the scapula with regard to winging, tilting, or rotation relative to the other scapula (June 30, 2021 Blog). From there, moving superior along the vertebral border of the scapula can help identify myofascial trigger points in the rhomboids (medially) as you move towards the spine of the scapula. This is a helpful anatomic landmark for the palpation of the rotator cuff muscles. Superior is the supraspinatus which may be followed to the distal attachment of the greater tuberosity. In the process, you will pass the acromio-clavicular (A-C) joint which can be assessed for gapping and you can drop anterior/inferior onto the coracoid process (the attachment of the coraco-clavicular ligament, coraco-humeral ligament, short head of the biceps brachii). Coming back to the A-C joint, one can follow the clavicle medially to confirm boney integrity and also to move proximally to get a sense of sternoclavicular muscle tension.
Going back to the most lateral aspect of the spine of the scapula, one can follow the posterior glenoid rim by moving posterior and inferior. One is now in the region of the other 3 rotator cuff muscles: in order of superior to inferior….infraspinatus, teres minor, teres major. Identification of each of these muscles is important. The infraspinatus is immediately inferior to the spine of the scapula and as an external rotator, the tendon can be found attaching to the greater tuberosity. Likewise, the teres minor is an external rotator but can be differentiated from the teres major (internal rotator) by actively performing internal and external rotation of the shoulder.
One can then move superiorly, back to the posterior glenoid fossa and follow the glenohumeral joint line to assess for the presence of a sulcus or pain. Joint line pain may be indicative of a labral tear. Continuing anterior to the bicep brachii and coracobrachialis tendons can be confirmed with active elbow flexion.
Palpation may reveal things like pain, crepitis, swelling, temperature, and rents (divot in the tissue). All of these signs may help to provide some insight into the need for further clinical tests and measures. One should be careful to maintain consistent and deliberate pressure with very precise palpation. Having too many contacts can confuse the patient and skew the feedback received from the patient. Again, palpation is a valuable skill and clinicians should be encouraged to refine the technique to contribute to the diagnosis of a pathology.
For more cutting-edge orthopedic information on iOrtho+ PREMIUM Mobile App, please visit the learning modules at https://iortho.xyz/
If you would like to learn more about the Mobil-Aider orthopedic measurement device to quantify joint mobility, please visit: https://mobil-aider.com/