![]()

Wrist Mobilization Techniques
Whether one experiences a Colles fracture or carpal tunnel syndrome (CTS), immobilization has the potential to limit motion. Colles fractures, also known as a dinner fork deformity, were named after Dr. Abraham Colles in 1814 and is the most common fracture in US and Northern European women up to 75 years of age. Whereas carpal tunnel syndrome, a pathology compressing the median nerve, effects approximately 5% of the people in the USA. Both conditions activate the inflammatory process and can result in weeks of immobilization from casts or splints. The inflammatory process results in ischemia, metabolic disturbance, and cell membrane damage. This manifests as swelling, erythema, increased temperature, pain, and loss of function. The proliferation of fibrin clotting and a proliferation of fibroblasts can contribute to scar (adhesion) formation. Best results can be achieved when mobilization is started promptly after immobilization.
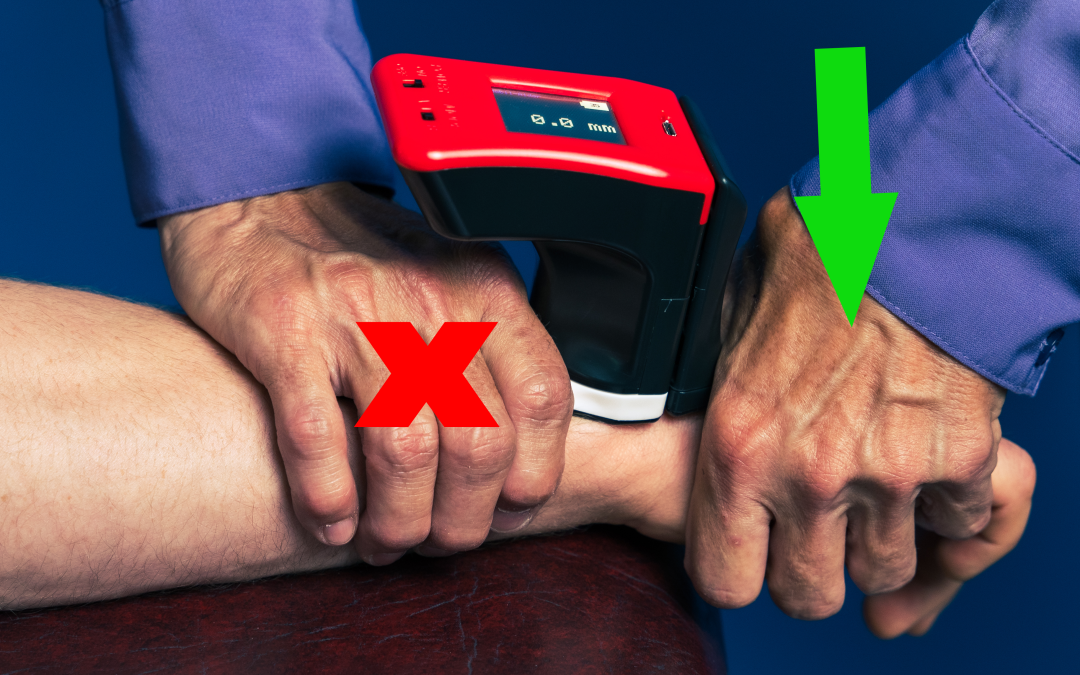
The arthrokinetic mobilizations that can help restore motion and strength are radiocarpal dorsal glides for flexion and volar glides for extension. The patient position for radiocarpal glides is seated with forearm supported and the wrist and hand off the edge of the surface. With the forearm supinated, the radius and ulna are stabilized proximally. The joint line is slightly over the edge of the table to allow for distal movement, and the proximal row of carpals is mobilized on the radius and ulna. The downward motion into a dorsal glide will facilitate flexion (left). If the forearm is pronated, the downward motion will facilitate extension (right). These movements are based on the concave-convex rule in which the convex proximal carpals roll and glide in the opposite direction on the concave radius.


Mobil-Aider device assists in the ability to quantify the small magnitude of movement (millimeters). For radiocarpal glides, the custom, dovetailed, white (H-F) attachment is donned. The white attachment is used to stabilize the radius and then the distal attachment is used to mobilize the proximal carpals. Then the mobilization techniques are exactly the same. Quantifying motion always the clinician to be consistent with a given mobilization grade and to assess the progression of the patient through the rehabilitation process.

 For more information in iOrtho+ Premium Mobile App, please visit: https://iortho.xyz/
For more information in iOrtho+ Premium Mobile App, please visit: https://iortho.xyz/
For more information on the Mobil–Aider and joint mobilization techniques, please visit the learning modules at https://iortho.xyz/
Subscriptions are only $1.99/month or $9.99/year. Over 450 clinical tests and over 120 manual techniques available via this WEB app – accessible on any device.
FYI – Prior blog posts are available at https://iortho.xyz/
Information on the Mobil-Aider Arthrometer to quantify joint mobility can be found at https://iortho.xyz/
- Gulick https://iortho.xyz/DT. iOrtho+ Premium Web App. DTG Enterprises LLC, 2025
- Wise CH, Gulick DT. Mobilization Notes. FA Davis Publishing, Philadelphia, 2009