The Knee: More than a Hinge Joint


The knee is a hinge joint with two-degrees of freedom: flexion/extension and rotation. With the concave tibial plateau and convex femoral condyles, open kinetic chain knee mobility involves rolling/gliding of a concave surface on a convex surface. Based on the convex/concave rule, rolling and gliding will occur in the same direction. Thus, to facilitate knee extension, one would perform an anterior glide and a posterior glide would facilitate knee flexion.
Knee Extension
 Anterior knee glides can be performed in either supine or prone positions. Biomechanically, it is always better to “push” than to “pull.” However, not everyone can assume a prone position to allow the clinician to “push,” so supine might be a necessity. In the supine position, one should place a small bolster or rolled towel under the knee to achieve a loose-packed position. An anterior glide can be performed by stabilizing the femur just above the knee and grasping the proximal posterior tibia/fibula to translate the lower leg anterior (Wise & Gulick, 2009). Care should be taken to try to keep your forearm in alignment with the direction of pull, i.e. parallel to the surface of the tibia.
Anterior knee glides can be performed in either supine or prone positions. Biomechanically, it is always better to “push” than to “pull.” However, not everyone can assume a prone position to allow the clinician to “push,” so supine might be a necessity. In the supine position, one should place a small bolster or rolled towel under the knee to achieve a loose-packed position. An anterior glide can be performed by stabilizing the femur just above the knee and grasping the proximal posterior tibia/fibula to translate the lower leg anterior (Wise & Gulick, 2009). Care should be taken to try to keep your forearm in alignment with the direction of pull, i.e. parallel to the surface of the tibia.
Quantifying Knee Mobility
The Mobil–Aider is a device designed to enable the clinician to quantify joint mobilizations. For the knee, the RED (H-B) attachment is snapped into the dovetail slot. The straps of the Mobil–Aider The molded plastic attachments contour to the knee to distribute the forces and provide a comfortable experience for the patient. Like the technique without the device, the
clinician to quantify joint mobilizations. For the knee, the RED (H-B) attachment is snapped into the dovetail slot. The straps of the Mobil–Aider The molded plastic attachments contour to the knee to distribute the forces and provide a comfortable experience for the patient. Like the technique without the device, the  tibia is anteriorly translated on the stabilized femur. Thus, the learning curve to use the Mobil–Aider is minimal. A reading on the device screen is in millimeters of movement. If the device is in the “A” mode, the maximal reading will be held for several seconds for ease of reading. If in the “B” mode, the reading is a real-time measure to permit consistency of the joint mobilization in the range of the desired grade. In a recent study comparing injured to uninjured knees, a Lachman test with the Mobil–Aider that was 2.05 mm greater on the injured side correlated with a partial ACL tear on MRI and when the difference was 3.38 mm greater, there was a complete ACL tear (Hammoud, Palombaro, Gulick, 2022). This is very valuable information to quantify the magnitude of an injury.
tibia is anteriorly translated on the stabilized femur. Thus, the learning curve to use the Mobil–Aider is minimal. A reading on the device screen is in millimeters of movement. If the device is in the “A” mode, the maximal reading will be held for several seconds for ease of reading. If in the “B” mode, the reading is a real-time measure to permit consistency of the joint mobilization in the range of the desired grade. In a recent study comparing injured to uninjured knees, a Lachman test with the Mobil–Aider that was 2.05 mm greater on the injured side correlated with a partial ACL tear on MRI and when the difference was 3.38 mm greater, there was a complete ACL tear (Hammoud, Palombaro, Gulick, 2022). This is very valuable information to quantify the magnitude of an injury.
When we talk about joint mobilization, Gorgos et al (2014) and Tragord et al (2013) have reported that skilled clinicians have good relative intra-clinician reliability, i.e. they could replicate their “force” application. This results in poor to moderate reliability between clinicians. Immediate visual feedback can enhance the consistency of the mobilization technique. Furthermore, mastering a psychomotor skill requires purposeful practice with visual feedback (Chang et al 2007; deSouza et al 2008). Concurrent feedback given while the learning task is in progress is critical (Chang et al 2007).
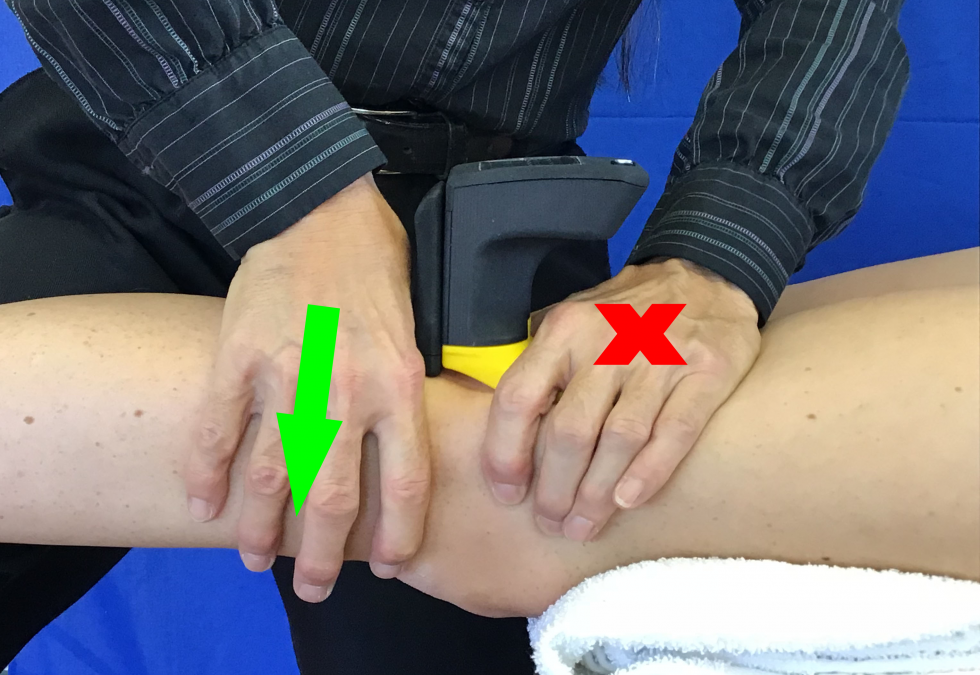
 When performing an anterior glide in prone, the bolster/towel roll is moved proximal so that it is under the anterior distal femur. This permits anterior tibial translation without compressing the patella. As shown, the clinician’s caudal hand cradles the distal tibia/fibula and the cephalad hand applies an anteriorly directed force to the posterior tibia. Once again, the clinician’s
When performing an anterior glide in prone, the bolster/towel roll is moved proximal so that it is under the anterior distal femur. This permits anterior tibial translation without compressing the patella. As shown, the clinician’s caudal hand cradles the distal tibia/fibula and the cephalad hand applies an anteriorly directed force to the posterior tibia. Once again, the clinician’s  forearm is in line with the direction of force, i.e. parallel to the tibial joint surface (Wise & Gulick, 2009). To use the Mobil–Aider device, one would don the yellow (H-C) attachment to stabilize the proximal joint surface and perform an anterior glide to the distal segment.
forearm is in line with the direction of force, i.e. parallel to the tibial joint surface (Wise & Gulick, 2009). To use the Mobil–Aider device, one would don the yellow (H-C) attachment to stabilize the proximal joint surface and perform an anterior glide to the distal segment.
The advantage of the prone glides are that it is easier for the clinician to push than to pull, gravity provides assistance to the mobilization, and the patient can work with you to actively extend the knee during the technique. When the patient works with the clinician to extend the knee, this is called “mobilization with movement.” In addition, in the prone position, the clinician can isolate the medial tibial plateau to apply the anterior glide asymmetrically. This will result in a lateral rotation of the tibia and replicate the “screw-home” mechanism of terminal knee extension.
Knee Flexion
Posterior glides of the tibia on the femur are used to facilitate knee flexion. If performed in supine, a bolster/towel roll is placed under the knee. The clinician stabilizes the thigh and the proximal tibia is translated posteriorly (Figure 6). Consistent with the concept of mobilization with movement, this technique can also be performed with increasing degrees of knee flexion (Wise & Gulick, 2009).
Recap
In summary, knee mobilizations can be valuable in reducing pain and restoring function. Moss et al (2007) reported knee mobilizations in the osteoarthritic patient produced both local and widespread hypoalgesic effects. This can be effective in reducing pain and mitigate the need for pain medication. Restoring arthrokinematic motion with mobilization techniques are important for improving joint range of motion and ultimately regaining muscle strength.
To download iOrtho+ Premium Mobile App, visit https://iortho.xyz
For more information on the Mobil–Aider or joint mobilization techniques, please visit the learning modules at https://mobil-aider.com/
- Chang J-Y, Chang G-L, Chang Chien C-J, Chung K-C, Hsu A-T. Effectiveness of two forms of feedback on training of a joint mobilization skill by using a joint translation simulator. Physical Therapy. 2007;87:418-430
- deSouza MS, Venturini C, Teixeira LM, Chagas MH, deResende MA. Force-displacement relationship during anteroposterior mobilization of the ankle joint. Journal of Manipulative & Physiological Therapeutics. 2008;31:285-292
- Gorgos KS, Wasylyk NT, Van Lunen BL, Hoch MC. Inter-clinician & intra-clinician reliability of force application during joint mobilization: A systemic review. Manual Therapy. 2014;19:90-96
- Gulick DT. iOrtho+ Mobile App. DTG Enterprises LLC, 2020
- Moss P, Sluka K, Wright A. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia. Physiotherapy. 2007;12(2):109-119
- Tragord BS, Gill NW, Silvernail JL, Teyhen DS, Allison SC. Joint mobilization force & therapist reliability in subjects with knee osteoarthritis. Journal of Manipulative & Physiological Therapeutics 2013;21(4):196-206
- Wise CH, Gulick DT. Mobilization Notes. FA Davis Publishing, Philadelphia, 2009